Shoulder dystocia Definition
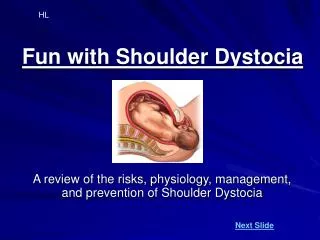
Shoulder dystocia Definition Failure of the shoulders to traverse the pelvis spontaneously after birth of the head -The anterior shoulder becomes trapped behind or on the symphysis pubis, while the posterior shoulder may be in the hollow of the sacrum or high above the sacral promontory.

Shoulder dystocia Definition
E N D
Presentation Transcript
Shoulder dystocia • Definition • Failure of the shoulders to traverse the pelvis spontaneously after birth of the head • -The anterior shoulder becomes trapped behind or on the symphysis pubis, while the posterior shoulder may be in the hollow of the sacrum or high above the sacral promontory
- a bony dystocia, impact the anterior shoulder, impeding attempts at delivery. • Figure 33.4 Shoulder dystocia.
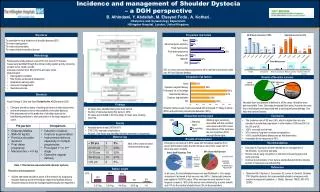
Risk factorsAntenatal • - high parity • - maternal age over 35 • - maternal obesity (weight over 90 kg). • -Fetal macrosomia (birth weight over 4000 g) has been associated with an increased risk of shoulder dystocia • - the incidence increasing as birth weight increases • -Maternal diabetes and gestational diabetes • -In diabetic women, a previous birth complicated by shoulder dystocia increases the risk of recurrence
In labor: • -post-term pregnancy • -oxytocin augmentation • -prolonged labour, prolonged second stage of labour • - operative deliveries
Warning signs and diagnosis • -The birth may have been uncomplicated initially, but the head may have advanced slowly and the chin may have had difficulty in sweeping over the perineum. • -Once the head is born, it may look as if it is trying to return into the vagina, which is caused by reverse traction. • -Shoulder dystocia is diagnosed when manoeuvres normally used by the midwife fail to assist the birth
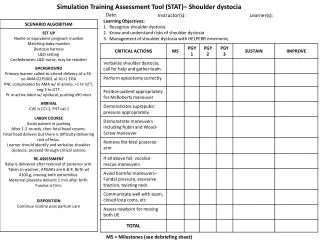
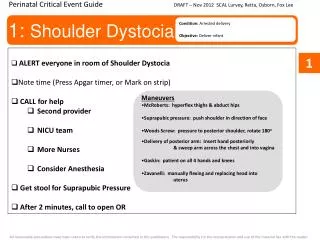
Management • . An obstetrician, an anaesthetist and a person proficient in neonatal resuscitation should be called. • Box 33.2 HELPERR mnemonic • Help • Episiotomy need assessed • Legs in McRoberts position • Pressure suprapubically • Enter vagina (internal rotation) • Remove posterior arm • Roll the woman over and try again
-Shoulder dystocia is a frightening experience for the mother, for her partner and for the midwife. • -The midwife should keep calm and try to explain as much as possible to the mother to ensure her full cooperation for the manoeuvres that may be needed to complete the birth. • -The purpose of all these manoeuvres is to disimpact the shoulders. The principle of using the most simple manoeuvres first should be applied.
-The midwife will need to make an accurate and detailed record of the type of manoeuvre(s) used and the time taken, • - the amount of force used • - and the outcome of each manoeuvre attempted.
Non-invasive proceduresChange in maternal position • -Any change in the maternal position may be useful to help release the fetal shoulders as shoulder dystocia is a mechanical obstruction. • -certain manoeuvres have proved useful
The McRoberts maneuver • -This manoeuvre involves helping the woman to lie flat and to bring her knees up to her chest as far as possible • -This manoeuvre will rotate the angle of the symphysis pubis superiorly and use the weight of the mother's legs to create gentle pressure on her
abdomen, • releasing the impaction of the anterior shoulder • -It is the maneuver associated with the lowest level of morbidity and requires the least force to assist the birth – • Suprapubic pressure • -Pressure should be exerted on the side of the fetal back and towards the fetal chest. • - This maneuver may help to adduct the shoulders and push the anterior shoulder away from the symphysis pubis into the larger oblique or transverse diameter
All fours position • -The all-fours position (or Gaskin manoeuvre) is achieved by assisting the mother onto her hands and knees • - the act of turning the mother may be the most useful aspect of this manoeuvre • -. In shoulder dystocia, the impaction is at the pelvic inlet and the force of gravity will keep the fetus against the anterior aspect of the mother's uterus and pelvis.
- However, this manoeuvre may be especially helpful if the posterior shoulder is impacted behind the sacral promontory as this position optimizes space available in the sacral curve and may allow the posterior shoulder to be delivered first- all fours maneuver, 83% of women were delivered with no other manoeuvres required • -Manipulative manoeuvres can be performed while the woman is on all fours but clear verbal communication is needed as eye contact is difficult
Manipulative procedures • Where non-invasive procedures have not been successful, direct manipulation of the fetus must now be attempted. • Positioning of the mother • -The McRoberts position • - the mother could be placed in the lithotomy position with her buttocks well over the end of the bed so that there is no restriction on the sacrum. • - If neither the McRoberts nor lithotomy positions are appropriate, then the all-fours position may prove useful. • - Any of the following manoeuvres can be undertaken with the mother in one of these positions.
Episiotomy • -The problem facing the midwife is an obstruction at the pelvic inlet which is a bony dystocia, • - Although episiotomy will not help to release the shoulders per se, the midwife should consider the need to perform one to gain access to the fetus without tearing the perineum and vaginal walls.
Rubin's manoeuvre • -This maneuvers (Rubin 1964) requires the midwife to identify the posterior shoulder on vaginal examination • - Then to push the posterior shoulder in the direction of the fetal chest, thus rotating the anterior shoulder away from the symphysis pubis. • - By adducting the shoulders this maneuvers reduces the 12 cm bisacromial diameter
Woods' maneuvers • -Woods' (1943) maneuvers requires the midwife to insert her hand into the vagina and identify the fetal chest. • - Then, by exerting pressure on to the posterior fetal shoulder, rotation is achieved. • - Although this maneuvers does abduct the shoulders, it will rotate the shoulders into a more favorable diameter and enable the midwife to complete the birth
Delivery of the posterior arm • -The midwife has to insert her hand into the vagina making use of the space created by the hollow of the sacrum • -Then two fingers splint the humerus of the posterior arm • - flex the elbow and sweep the forearm over the chest to deliver the hand • -If the rest of the birth is not then accomplished, the second arm can be delivered following rotation of the shoulder using either Woods' or Rubin's manoeuvre or by reversing the Løvset manoeuvre
Zavanelli manoeuvre • -If the manoeuvres described above have been unsuccessful, the obstetrician may consider the Zavanelli manoeuvre (Sandberg 1985) as a last hope for birth of a live baby. • -The Zavanelli manoeuvre requires the reversal of the mechanisms of birth so far and reinsertion of the fetal head into the vagina. Delivery is then completed by caesarean section. • -The head is returned to its pre-restitution position • -. Pressure is then exerted on-to the occiput and the head is returned to the • -Prompt delivery by caesarean section is then required.
Symphysiotomy • -Symphysiotomy is the surgical separation of the symphysis pubis • - used to enlarge the pelvis to enable the birth. • -It is usually performed in cases of cephalopelvic disproportion • - d is used more routinely in the developing world. • -There are a few recorded cases where symphysiotomy has been used successfully to relieve shoulder dystocia • -but the procedure has usually been associated with a high level of maternal morbidity. • -The rarity of reported cases makes it difficult to assess the technique for the relief of shoulder dystocia.
Outcomes following shoulder dystocia • Maternal • -Approximately two-thirds will have a blood loss of >1000 mL from injury associated with the birth • -Maternal death from uterine rupture has been reported following the use of fundal pressure • - Hemorrhage during and following the birth • Fetal • -Neonatal asphyxia the attending pediatrician must be experienced in neonatal resuscitation • -Brachial plexus injury with damage to cervical nerve roots 5 and 6 may result in an Erb's palsy). • .
-This is commonly associated with shoulder dystocia when the head and neck have been twisted and pulled • -Neonatal morbidity may be as high as 42% following shoulder dystocia
- Fetal damage may occur even with excellent management using appropriate obstetric manoeuvres • -Shoulder dystocia remains a cause of intrapartum fetal death • -The midwife must ensure that she takes opportunities to practice the practical skills needed to complete a birth complicated by shoulder dystocia. • - Mannequins may help in simulation training and practice drills.