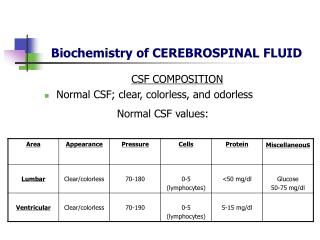
Download
1 / 42
430 likes | 751 Views
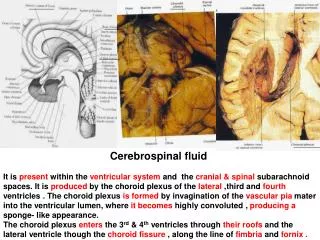
Cerebrospinal Fluid Studies in MSA Nadia Magdalinou Clinical Research Fellow 27.02.14. Pathophysiology. Protein misfolding and pathological aggregation are common threads in neurodegeneration. α- Syn deposition in MSA. Tau deposition in PSP. Courtesy of Dr Janice Holton.

E N D
Cerebrospinal Fluid Studies in MSANadia MagdalinouClinical Research Fellow27.02.14
Pathophysiology Protein misfolding and pathological aggregation are common threads in neurodegeneration α-Syn deposition in MSA Tau deposition in PSP Courtesy of Dr Janice Holton
Overlapping Pathologies & Phenotypes in “Proteinopathies” Adapted from Constantinescu and Mondello 2013
Biomarker “a characteristic that is objectively measured and evaluated as an indicator of normal biological processes, pathogenic processes or pharmacologic response to a therapeutic intervention” (Biomarkers Definitions Working 2001) ‘Ideal’ biomarker: • sensitive • reproducible • closely associated with the disease process • non-invasive and inexpensive
Cerebrospinal fluid • proximity to brain structures undergoing degeneration • Proteins/peptides directly reflective of disease pathology would most likely diffuse into the CSF than any other fluid • can be tested serially; assessing evolving pathology throughout the disease course
CSF studies in Parkinsonism Main focus to investigate a priori defined compounds (hypothesis-driven) • in patients and in healthy controls • looking for differences, patterns and associations; α-Syn, tau Recently, trend towards hypothesis-generating, “omics” techniques • unbiased and sensitive approach • identifying markers unexpectedly involved in neurodegeneration Even though several promising candidates exist there is still no reliable biomarker
Putative pathogenic pathways underlying CSF Biomarkers in PD Parnetti, L. et al. Nat Rev.Neurol. 9, 131-140 (2013)
Total-α-Syn(Magdalinou, Lees, Zetterberg, JNPP 2014 in press) • Inconsistent initial data • Consensus emerging: decreased in DLB, PDD, PD and MSA, but not in PSP and CBD • Can differentiate synucleinopathies from tauopathies and controls • Cannot discriminate between synucleinopathy groups
Putative pathogenic pathways underlying CSF Biomarkers in PD Parnetti, L. et al. Nat Rev.Neurol. 9, 131-140 (2013)
Phosphorylated (p-α-Syn) and Oligomeric α-syn (o-α-Syn) • Wang: p-α-Syn:t-α-Syn ratio could discriminated MSA from PSP • Foulds: o-p-α-Syn can differentiate MSA from other synucleinopathies and tauopathies • No correlation with age/disease duration/cognitive function
Putative pathogenic pathways underlying CSF Biomarkers in PD
Total & Phosphorylated Tau • Inconsistent data • Can discriminate PD from AD • No difference in parkinsonian conditions • Age, not diagnosis, strongest factor affecting t-tau levels
Neurofilament-light chain • NF-L normal in PD and increased in MSA, PSP and CBD vs controls • No difference in atypical parkinsonism • Levels remain stable despite disease progression in a longitudinal study
Putative pathogenic pathways underlying CSF Biomarkers in PD Parnetti, L. et al. Nat Rev.Neurol. 9, 131-140 (2013)
Oxidative Stress Markers • DJ1: inconsistent results; ? Increase in MSA could differentiate MSA from PD • Urate: inconsistent results
Inflammatory Markers MSA and PD could be differentiated by the CSF Fractalkine and not by α-Syn
Challenges/Limitations • Most studies are retrospective and do not have pathological confirmation • Lack of standardisationof pre-analytical (sampling collection, handling and storage) and analytical (analysis execution/sample processing) factors • Lack of assay standardisation; different assays can give different absolute concentrations of the protein, making it almost impossible to use global reference limits and diagnostic cut-off points • Heterogeneous neurodegenerative groups: in terms of age, disease duration and disease severity • Heterogeneous controls groups: including healthy controls, patients with non-neurodegenerative neurological conditions or patients with possible neurodegenerative conditions like mild cognitive impairment and normal pressure hydrocephalus • Lack of combination of different biomarker modalities- imaging and CSF markers
Methods • Prospective, cohort study of patients with parkinsonian conditions, healthy and dementia controls recruited from NHNN • Patients monitored periodically for at least two years to maximise accuracy of clinical diagnosis • Dx according to current consensus criteria • Healthy controls with no history of neurological/psychiatric disease Hypothesis Parkinsonian syndromes can be differentiated using a combination of targeted cerebrospinal fluid markers A subgroup of participants underwent brain imaging to assess whether the combination of multiple modalities improves diagnostic accuracy • Standardised protocol for the collection and storage of CSF (as recommended by the Alzheimer’s Association QC Program for AD) and sample processing • ≈50% of participants have signed up for brain donation and we have already pathological confirmation in 10 patients
MCP-1 and YKL-40 sAPPα and sAPPβ 2 soluble metabolites resulting from proteolytic processing of Amyloid Precursor Protein (APP) sAPPα and sAPPβ unaltered in AD, but not investigated in other neurodegenerative conditions • Monocyte Chemoattractant Protein-1: a small cytokine • YKL-40:a secreted glycoprotein named after its three terminal amino acids • involved in neuroinflammatory processes associated with neurodegeneration in AD • Decreased levels of YKL-40 in synucleinopathies compared with tauopathies and healthy controls (Olsson et al 2013)
Final number of subjects included in the analysis DISEASED SUBJECTS HEALTHY CONTROLS
Demographic and Clinical Characteristics • no significant age difference in parkinsoniansyndromes • significant difference in disease duration between the PD group and the rest • significant difference in H&Y score between PSP and MSA, PD and ‘unclassifiable’ • no significant difference in UPDRS • significant difference in MMSE scores between PD and controls
‘Dementia’ Markers Aβ42, t-tau and p-tau showed a significant difference between AD and all other groups, but did not discriminate between parkinsoniansyndromes
Targeted Markers • Significant reduction in MSA compared with healthy controlsand AD • No significant difference in PD
Targeted Markers • There was a significant increase in all studied groups compared with healthy controls • PSP, CBS and MSA pts had higher levels compared with PD, AD, FTD and Unclassifiable pts
Targeted Markers • There was a significant difference between healthy controls and all studied groups • In PSP there were significant higher levels compared with FTD
Targeted Markers • Healthy controls had significantly lower levels compared with PSP, MSA and Unclassifiable pts • There were higher levels in CBS compared with PD and Unclassifiable pts
Targeted Markers • Healthy controls had significantly higher levels compared with PSP, MSA and CBS • PSP, CBS and MSA had significantly lower levels compared with PD and AD
Targeted Markers • Healthy controls had significantly higher levels compared with atypical parkinsonian groups • Atypical parkinsonian groups had lower levels compared with PD, but there were no differences between them • PSP had lower levels compared with AD
Summary Summary
Conclusion • Unpublished data • Preliminary analysis only • Promising early results: reproduced other published data • Unlikely that a single biomarker will hold the answer: combination of markers may be required
Proteomics • protein content (proteome) of a sample is characterised • proteomes between patients and controls are compared and differences are identified Technology: • separation of proteins • analysing proteins through mass spectrometry • quantifying and identifying proteins through advanced data processing
Proteomics Studies Limitations: inherently biased towards identification of abundant proteins blood contamination in CSF major effect on protein concentration not standardised sample preparation/implementation and processing technologies between research groups difficult to validate and replicate results
Proteomics Hypothesis Cerebrospinal fluid proteomic patterns can discriminate between parkinsoniansyndromes
Discovery Cohort Results • Immunoglobulinsuperfamilymember8Fragment • Amyloidlikeprotein1OSHomosapiensGNAPLP1PE4SV • NeurosecretoryproteinVGFOSHomosapiensGNVGFPE1 • EndothelinBreceptorlikeprotein2OSHomosapiensGN • Scrapieresponsiveprotein1OSHomosapiensGNSCRG1P • Lymphocyteantigen6HOSHomosapiensGNLY6HPE2SV1 • Isoform2ofCalsyntenin1OSHomosapiensGNCLSTN1 • HaptoglobinOSHomosapiensGNHPPE1SV1HPT_HUMA • Alpha1antichymotrypsinOSHomosapiensGNSERPINA3PE • ComplementC3OSHomosapiensGNC3PE1SV2CO3_HU • Iggamma4chainCregionOSHomosapiensGNIGHG4PE1 • Collagenalpha1IchainOSHomosapiensGNCOL1A1PE • ApolipoproteinEOSHomosapiensGNAPOEPE1SV1A • Isoform2ofFibrinogenalphachainOSHomosapiensG • IsoformGammaAofFibrinogengammachainOSHomosap • ProteinAMBPOSHomosapiensGNAMBPPE1SV1AMBP • Isoform2ofMajorprionproteinOSHomosapiensGNP • Alpha1BglycoproteinOSHomosapiensGNA1BGPE1SV4 • IgkappachainVIIIregionVGFragmentOSHomosapie • Secretogranin1OSHomosapiensGNCHGBPE1SV2S • Heparincofactor2OSHomosapiensGNSERPIND1PE1SV • Isoform2ofGelsolinOSHomosapiensGNGSNGELS • MonocytedifferentiationantigenCD14OSHomosapiensG • ComplementcomponentC7OSHomosapiensGNC7PE1SV2 • ChromograninAOSHomosapiensGNCHGAPE1SV7CMG • Secretogranin2OSHomosapiensGNSCG2PE1SV2SC • Insulinlikegrowthfactorbindingprotein2OSHomosa • Fibulin1OSHomosapiensGNFBLN1PE1SV4FBLN1_H • IsoformCofFibulin1OSHomosapiensGNFBLN1FB • PeptidylprolylcistransisomeraseBOSHomosapiensG • Insulinlikegrowthfactorbindingprotein6OSHomosa • Zincalpha2glycoproteinOSHomosapiensGNAZGP1PE1 • Phosphatidylethanolaminebindingprotein1OSHomosapi • SerumamyloidA4proteinOSHomosapiensGNSAA4PE1 • Chitinase3likeprotein1OSHomosapiensGNCHI3L1PE • ProstaglandinH2DisomeraseOSHomosapiensGNPTGDSP • CellsurfaceglycoproteinMUC18OSHomosapiensGNMCAM • LumicanOSHomosapiensGNLUMPE1SV2LUM_HUMAN • LysozymeCOSHomosapiensGNLYZPE1SV1LYSC_HUM • Isoform2ofEGFcontainingfibulinlikeextracellula • ProcollagenCendopeptidaseenhancer1OSHomosapiens • Extracellularmatrixprotein1OSHomosapiensGNT • Metalloproteinaseinhibitor1OSHomosapiensGNT • InteralphaGlobulininhibitorH2OSHomosapiensGN • Vsetandtransmembranedomaincontainingprotein2AOS • Secretogranin3OSHomosapiensGNSCG3PE1SV3SC • ProteinFAM3COSHomosapiensGNFAM3CPE1SV1FAM • Neuralproliferationdifferentiationandcontrolprotei
Conclusion • Early and accurate diagnosis in MSA is very important, esp with emergence of disease modifying drugs • Clinical diagnosis is inaccurate, particularly in the early stages • ‘Holy grail’- accurate diagnostic test • Remains elusive; on-going work with established, hypothesis testing biomarkers and hypothesis generating markers from proteomics studies • Combination of markers may be required
Acknowledgements DRC Jason Warren Nick Fox Cath Mummery Jon Schott Martin Rossor Ross Paterson Jamie Toombs Katie Judd Gothenburg Henrik Zetterberg Johan Gobom Max Petzold • NHNN • Henry Houlden • Nick Wood • Kailash Bhatia • Patricia Limousin • Tom Foltynie • Simon Farmer • Paul Jarman • Paola Giunti • Chris Mathias • Gordon Ingle • Lucia Schottlaender • Mike Lunn • Miles Chapman RLWI Andrew Lees Tom Warner John Hardy Rohan de Silva Janice Holton Helen Ling AtbinDjamshidian Alastair Noyce Karen Doherty GeshantiHonhamuni Connie Luk IliyanaKomsiyska Karen Shaw Funding: PSP association, RLWI, Wolfsonfoundation award