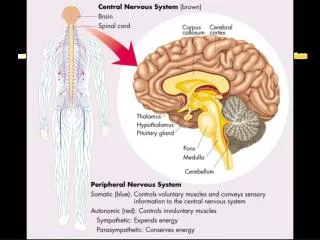
Peripheral Nervous System
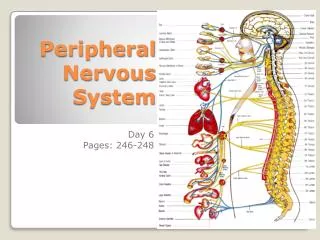
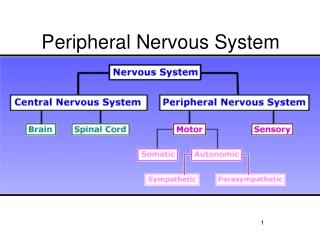
Brain. Spinal Cord. Nerves. Peripheral Nervous System. 3 kinds of neurons connect CNS to the body sensory motor interneurons Motor - CNS to muscles and organs Sensory - sensory receptors to CNS Interneurons: Connections Within CNS. Brain. Sensory Neuron. Motor Neuron.


Peripheral Nervous System
E N D
Presentation Transcript
Brain Spinal Cord Nerves Peripheral Nervous System • 3 kinds of neurons connect CNS to the body • sensory • motor • interneurons • Motor - CNS to muscles and organs • Sensory - sensory receptors to CNS • Interneurons: Connections Within CNS
Brain Sensory Neuron Motor Neuron Skin receptors Interneuron Muscle Somatic System • Nerves to/from spinal cord • control muscle movements • somatosensory inputs • Both Voluntary and reflex movements • Skeletal Reflexes • simplest is spinal reflex arc
Somatosensation • The sensations caused by the stimulation of receptors in the skin. 1) tactile: fine touch, crude touch, deep touch/pressure, vibration, flutter, skin indentation, etc 2) pain: mechanical pain such as cutting and heat-pain 3) thermal senses: mediates warm and cold, but not heat-pain 4) proprioception/kinesthesis: sense of muscle and joint position for static (stationary) and dynamic (moving) limbs
Touch • Touch is a very general term used to refer to somatosensation, sensations due to: • Mechanical displacement of the skin - permitting awareness of the environment and things that are in contact with the body, producing pleasurable or uncomfortable sensations that promote or inhibit contact with various other objects or organisms • Temperature and changes in temperature - permitting organisms to find comfortable or tolerable temperatures • Pain as a result of damage to tissues - warning an organism about injury and illness, in concert with the awareness of mechanical displacement and temperature: the ability to determine the direction that harm is coming from and producing reflexive movements to minimize harmful contacts • Mechanical displacement or stretching of muscles, tendons and joints (kinesthesis) - permitting an organism detailed knowledge about where various body structures are in relation to each other, movement relative to each other and the external environment, how much work muscles are doing and whether they or their associated tissues are in danger of overwork or injury (this last is in concert with pain receptors) • Sensation of direction changes and orientation relative to gravity (vestibular) - assists the organism in visual perception of movement, awareness of own movement • These last two, of which people are generally not aware, are collectively called proprioception
Four receptors Meissner corpuscle Merkel receptor Pacinian corpuscle Ruffini cylinder
Tactile acuity and Receptive fields RF neuron
Pathway Two pathways: 1) Medial lemniscal pathway: large fibers carry signals related to sensing the positions of the limbs (proprioception) and perceiving touch. 2) Spinothalamic pathway: small fibers transmit signals related to temperature and pain.
Gross Brain Structure & Function Cerebral Cortex Our body is ‘mapped’ on the Motor and Somatosensory Cortex (area on sensory or motor cortex related to amount of innervation)
Pain Perception • Receptors: Nociceptors • Two types of sensory nerve fibers transmit signals that the brain interprets as pain. • Aδ ("A-delta") fibers • These are thinly-myelinated. • Their activation is rapid and associated with acute pain. This is "good pain" because it warns you to do something to take care of the problems, e.g., a hot saucepan. • C fibers • These are unmyelinated and thus conduct impulses slowly. • Their activation is slower and associated with diffuse, dull, chronic pain. This is "bad pain" because it cannot be alleviated simply by removing the stimulus. It is pain generated by such things as damaged tissue and cancer.
Controlling Pain • Fear, or high levels of anxiety, almost always increase pain • If you can regulate a painful stimulus, you have control over it • Distraction can also significantly reduce pain • The interpretation you give a stimulus also affects pain
Coping With Pain • Prepared Childbirth Training: Promotes birth with a minimal amount of drugs or painkillers • Counterirritation: Using mild pain to block more intense or long-lasting pain
Pain • Phantom Limb: Missing limb feels like it is present, like always, before amputation • Visceral Pain: Pain fibers located in internal organs • Referred Pain: Pain felt on surface of body, away from origin point • Somatic Pain: Sharp, bright, fast
Gate Control Theory of Pain • Gate Control Theory: Pain messages from different nerve fibers pass through the same “neural” gate in the spinal cord. • If gate is closed by one pain message, other messages may not be able to pass through
Adaptation, Attention, and Sensory Gating • Sensory Adaptation: When sensory receptors respond less to unchanging stimuli • Selective Attention: Voluntarily focusing on a specific sensory input • Sensory Gating: Facilitating or blocking sensory messages in spinal cord
Fig. 5.32 A sensory gate for pain. A series of pain impulses going through the gate may prevent other pain messages from passing through. Or pain messages may relay through a “central biasing mechanism” that exerts control over the gate, closing it to other impulses.
Types of Pain • Warning System: Pain carried by large nerve fibers; sharp, bright, fast pain that tells you body damage may be occurring (e.g., knife cut) • Reminding System: Small Nerve Fibers: Slower, nagging, aching, widespread; gets worse if stimulus is repeated; reminds system that body has been injured
Pain • Pain is an essential sensation to our survival. Loss of sensation to a region makes it surprisingly easy to severely damage the body and not notice. This is particularly important in working with patients with spinal cord damage. • Pain projection is less straightforward than touch or proprioception, and is far less well understood. Perception of pain can be altered by many things, including affect - fear and anxiety enhance pain, whilst pain thresholds in relaxed individuals can be far greater. • Nociceptors are responsive to a wide range of stimuli, including several paracrine agents released in response to injury, inflammation or infection. In addition, they are sensitive to substance P, which is released when by recurrent collaterals if the nociceptor is stimulated for long enough. This can lead to the phenomenon of 'wind-up' - and is why local anaesthetics are frequently applied to an area being operated on even when a general anaesthetic is already in use. Substance P has this effect both centrally and peripherally. • Prostaglandins may sensitise nociceptors - however, there is probably a central role of these agents in pain as well, and paracetamol has been suggested to act mainly through a hypothesised COX-C enzyme in the CNS (if only because its role is harder to define than NSAIDs such as aspirin…). Noxious heat is detected by a receptor thought to be a homologue of 'trp' in drosophila - 'trp-like', or trpl receptors. This is also sensitive to capsaicin. • These effects taken together lead to hyperalgesia - in addition, normally non-noxious stimuli can become painful, a process called allodynia. • Pain undergoes some form of afferent gating in the substantia gelatinosa. The original Melzack and Wall theory fails to explain some observations related to pain - but does explain allodynia. The most likely solution is probably a combination of their ideas with more recent 'wiring diagrams' that give a greater role to the substantia gelatinosa and descending projections from the midbrain. An interesting observation in support of gating is that a very local warm stimulus often feels painful where a larger one merely feels warm - i.e. the larger one provides more non-painful input… • It is unclear how pain is localised. Visceral pain tends to be felt in the region of skin supplied by the same nerves (as this related to the embryological position of development of the organ, the pain can be referred distantly - e.g. heart pain to the shoulders, appendix pain to the navel, and in men testicular pain to the upper abdomen). Localisation of pain on the skin is probably aided by touch information, and probably prior expectation. • Pain can undergo a large degree of descending control. The main source of inhibition of pain signals is the periaqueductal grey matter (PAG) in the midbrain, which projects both upwards and downwards, and releases enkephalin and other endogenous opioids. Morphine is still one of the most widely used drugs to control severe pain in humans. Recent experiments suggest that this control can be targeted to individual areas. • Hypnosis can also be used to control pain - the effect of this is not greatly altered by opioid antagonism (e.g. Naloxone), and may involve the production of a dissociated state in which pain exists but is not felt as a 'bad thing', or associated with one's own body. Contrast this with placebo pain reduction, which is blocked by nalaxone.
Fig.5.28 Visceral pain often seems to come fro mthe surface of the body, even though its true origin is internal. Referred pain is believed to result from the fact that pain fibers from internal organs enter the spinal cord at the same location as sensory fibers from the skin. Apparently, the brain misinterprets the visceral pain messages as impulses from the body’s surface.
Analgesic substances • Endorphins: neurotransmitters found in the brain that have pain-relieving properties similar to morphine. There are three major types of endorphins: beta endorphins, found primarily in the pituitary gland; and enkephalins and dynorphin, both distributed throughout the nervous system.