Establishing Goals of Care
470 likes | 502 Views
This session will enhance learners' ability to discuss goals of care with patients facing serious health conditions. Topics include surrogate decision-making, prognosis, and end-of-life planning. Participants will practice essential communication components through simulations to gain confidence. Key elements involve understanding prognosis, clarifying misunderstandings, identifying goals, and creating care plans. The presentation explores barriers to effective communication and decision-making at the end of life. Studies on CPR depiction in TV shows and patient preferences regarding resuscitation will be discussed, alongside important issues like advanced directives and knowledge gaps on end-of-life care. The session aims to improve competence in conducting goals of care conversations, focusing on patient-centered approaches and addressing common fears and misunderstandings.

Establishing Goals of Care
E N D
Presentation Transcript
Establishing Goals of Care Ed Martin, MD Revised by Sarah Rose Lamport RNP Alpert Medical School of Brown University
Speaker Disclosures • No financial disclosures
Goals of the Session At the end of this session, learners will be able to: • Be comfortable and effective in talking with patients and families about goals of care for patients with serious life-threatening, or chronic conditions • Describe goals of care discussions as an essential component of the practice of medicine accepted within the mainstream of legal, moral, and ethical principles • Articulate the complexity and subtleties of surrogate decision-making, and the concept of substituted judgment • Practice the key components of goals of care discussions in a simulation as a means of gaining competence and confidence in conducting GOC conversations
Key elements in a goals of care conversation • Determine understanding of prognosis • Clarify any misunderstanding • Identify goals of care • Develop plan of care based on the identified goals
Barriers to Communication and End of Life Decision Making • Misunderstandings re: limits of medical care (curative vs palliative treatments, multiple opinions) • Misunderstandings re: prognosis (mortality vs functional recovery, quality of life) • Misconceptions re: palliative care, hospice care, comfort measures
Cardiopulmonary Resuscitation on Television • Original study in NEJM in1999 looked at ER, Chicago Hope and rescue 911, 60 occurances in 97 episodes, 75 % survival rate, 67% survived to d/c • *** • Follow up study in Resuscitation in 2015 looked at House and Grey’s Anatomy and found that in the 2 seasons (91 episodes total) CPR was depicted 46 times, with a survival rate of 69.6%, of those 71.9% survived to discharge. Advanced directives were discussed for 2 patients. Diem SJ, Lantos JD, Tulsky JA, NEJM 1991;334:1578-82
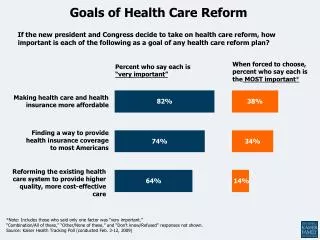
The Influence of the Probability of Survival on Patient’s Preferences Regarding CPR • 41% to 21% after learning probability of survival Murphy DJ, et al. NEJM 1994;330:545-49
Prognosis • Complex discussions may be difficult to reduce to percentages, but patients and families often wish to hear a number • Always remember to ask first • Nuances such as level of function if illness is survived must be conveyed
Epidemiology and Prognosis of Coma in Daytime Television Drama • Comas lasted median of 13 days • 89 % full recovery • 8% died • 3% vegetative state • Those that recovered, 86% had no deficits the day they regained consciousness Casarett D et al. BMJ. 2005;331:1537-9
Knowledge about end of life care • 69% correct about refusal of treatment • 46% about withdrawal of treatment • 23% assisted suicide • 32% active euthanasia • 41% double effect • 62% equated assisted suicide and euthanasia • More knowledge with white race, college degree, having served as a surrogate decision maker • Not associated with personal experience with illness, death or illness of loved one, authoring an advanced directive Silveira et al. JAMA. 2000; 284:2483-8
Words that can have a negative impact • “There is nothing more to do” • “Would you like us to do everything possible” • “Stop the machines” • “Withdrawal of Care” Pantilat SZ. JAMA.2009;301:1279-81
“There is Nothing More to Do” • “to cure the illness” • Not true • Feels like abandonment • Replace with “ I wish there were something we could do to cure your illness.” “Let’s focus on what we can do to help you.”
“Would You Like Us to Do Everything Possible” • “to help you achieve your goal”, “that would be helpful given the circumstances” • What is everything?
Patients who want everything • Everything that might provide maximum relief of suffering, even if it might unintentionally shorten life • Everything that has any possible potential to prolong life even a small amount, regardless of its effect on the patient’s suffering Quill,TE et al. Ann Intern Med 2009;151:345-9
“Stop the Machines” • Focuses on what will not be done • “To respect his wishes we will stop the breathing machine and make his breathing comfortable” • “If your heart stops we will let you die peacefully”
“Withdrawal of Care” • Care is never withdrawn although certain interventions may be. • “Withdrawal of mechanical ventilation and vasopressors and institution of comfort measures”
Fears • Abandonment • Providers may be less likely to provide care unrelated to resuscitation • “What worries you the most” • “What are you hoping for”
Misunderstanding • “What is your understanding of your condition/prognosis.” • “What are your most important goals” • “Tell me more about what you mean by ‘everything’”
Faith • “Does your religion provide any guidance in these matters” • Offer chaplains
Family • “How is your family handling this.” • Identifying surrogate decision maker • Use of interpreters as indicated
Developing a Plan • Asking permission • Aligning intention • Provider may suggest a plan of care based on patient’s treatment philosophy and goals of care given the medical condition and prognosis. • Consider a time limited trial when there is disagreement regarding plan.
Harm-Reduction Strategy • When patient wants full care with no limits • Ongoing negotiation can feel like badgering • May still exercise clinical judgment i.e. stop CPR after one cycle. NOT a slow code. Or not offering CPR if medical team feels will harm patient without hope of benefit—Nonmaleficence • Support the care team who might also be struggling.
Use of Educational Videos • Research has shown videos can be more effective than verbal descriptions in conveying complex information and procedures i.e. CPR • Increase in concurrence of surrogates with decision making • Increased knowledge • Decrease uncertainty • Increase preference for comfort measures at end of life
Improving Do-Not-Resuscitate Discussions: A Framework for Physicians Taylor RM et al. J Supportive Oncol.2010;8:42-44
CPR • Otherwise healthy patient: arrest is cause of death, CPR treats cause • Dying patient: arrest is mechanism of death. CPR does not treat cause of death • “option” of resuscitation suggests it is an intervention that makes sense • DNR should be clearly recommended by physician for dying patient • Otherwise burden placed on family to refuse an intervention that makes no sense
“Informed Assent” • A tool you can use when discussing interventions that do not make clinical sense, eg: CPR in a dying patient, feeding tube in advanced dementia • Provide recommendation • Patient/surrogate can opt out
Getting Started • Privacy • Time for discussion • Are the people there who need to be there i.e. family, other caregivers • Explain this is a routine process and does not suggest death is imminent (if it is not) • Sometimes the patient may bring it up • Sometimes the patient may refuse to enter into a discussion
Getting started:Assess Understanding • What have your doctors told you about your condition? • What is your understanding of how things are going? • What were you expecting might happen at this point?
Getting started:Assess Understanding • May need to recalibrate, correct • “I spoke with your Doctor and this was my understanding of what she said.” • “I have had the chance to review the record and examine your mother and this is what I have found” • “I wish I had better news to give you.” • “I am worried the condition may be more severe than you have described” • Empathy crucial here and throughout • Avoid jargon and complex terminology
Advance Directives • Does the patient have an advance directive? • What does it say?
Family History • “Noncontributory” • What parents or other relatives died of often not helpful in this. • How they died and what patient thinks about that can be helpful. • Did they die in the hospital? • After a long ICU stay? • Did they die on a vent? • Did they have CPR after they died?
Social History • Number of siblings, tobacco history or alcohol history may be less important for goals of care • What is important to the patient may be revealed by some of the topics in this area i.e. occupation, hobbies..
Surrogacy • Family may have no idea about proper role of surrogate • In fact, they may have been asked “What do you want us to do for your mother.” “Do you want us to do everything for your father?”
Surrogacy • Is there an advance directive? • “You know your brother much better than we do. Can you tell us what he would have wanted if his illness had become this severe?” • “If your mother could sit up and tell us now what she would want us to do, what would she say?” • It may be helpful to explore what kind of person the patient was. What was important? Longevity?, Independence?
Assessing Values Oncotalk suggestions: • “As you think about the illness, what is the best and the worst that might happen?” • “What makes life worth living for you?” • “Would there be any circumstances under which you would find life not worth living?” • “Have you seen or been with someone who had a particularly good death or a particularly bad death?” • “How do you think about balancing quality of life with length of life in terms of your treatment?” Arnold, R. M., Back, A. T., Baile, W. F., Fryer-Edwards, K., & Tulsky, J. A. (2011). The Oncotalk model. In Handbook of Communication in Oncology and Palliative Care Oxford University Press.
Goals of Care • Discussion should never focus on presenting a checklist of medical interventions • Discussion should not focus on simply what will not be done • Focus should be on what will be most likely to help patient achieve their goals • Will need to confirm understanding of the possible consequences of preferences and decisions
Goals of Care • “What are you hoping for?” • Hope to elicit what the patients goals are and what they are willing to undergo to achieve that goal, their preferences for care • We can help educate regarding the reality of achieving a goal as well as help in determining the most effective way of achieving that goal
Goals of Care • Some patients are willing to undergo any treatment that has any chance to prolong life even a small amount, regardless of its causing suffering, even if it meant being kept alive on a machine, unaware of their surroundings. • Others are at a point in their lives where they just want to be kept comfortable. • Most patients are somewhere in between.
Goals of Care • Once goals of care are established, the team can begin to develop a plan that will help achieve those goals • Strong MD input is needed to insure the plan makes sense, i.e. do not hospitalize but full code does not make sense
Decision Making is a Process • Establishing goals of care is a critical step in this process • Will often not wrap it all up in one meeting • Discussion may evolve • First patient and family need to understand prognosis • Goals, values and decisions may change dramatically • Meet patient and family where they are at
Code Status • When patient and/or family are not ready to discuss GOC, but code status needs to be addressed • Seatbelt plan: “We don’t get into a car expecting to have an accident, but we wear a seatbelt “just in case”. Let’s work on a “just in case” plan for you. • Normalizing refusing medical interventions for different reasons
Palliative Care Consultation • Available and willing to assist with your difficult situations with patients and families • One caveat: avoid offering interventions you think make no sense • Most patients and families will think if you offer something you must think it is reasonable
Conclusions • Goals of care discussions are an essential component of the practice of medicine and are accepted within the mainstream of legal, moral, and ethical principles • Appropriate surrogate decision-making can help insure that the patient’s goals and values are identified and honored • Decision making is a process
FACULTY ROLE PLAY • Bad example • Better example
PARTICIPANT ROLE PLAY ClinicalScenario: This 82 year old male with Class IV CHF was admitted for treatment of pneumonia. His co-morbidities include COPD (not oxygen dependent), moderately severe dementia, and chronic kidney disease stage 4. He had been declining at home prior to admission and has now stopped eating. Workup did not identify any readily reversible problems for his decline. You have been asked to speak with the family to update them on his condition and discuss goals of care.
PARTICIPANT ROLE PLAY The 3 activities in order should be as follows: • Initiation of a GOC discussion: What is your understanding of what your doctor has told you? • Surrogate decision making discussion: If your family member could hear what we’ve discussed and the likely outcomes, what would she want? • Conclusion of the GOC discussion: Here’s what I’m hearing you say, and here is my recommendation.