Download
1 / 13
130 likes | 380 Views
Home Management of Malaria study. By Victor Chalwe , MD, MSC . ICIUM , Turkey. Introduction.

E N D
Home Management of Malaria study By Victor Chalwe, MD, MSC. ICIUM, Turkey
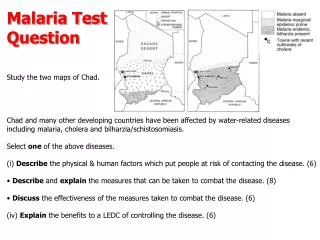
Introduction • The home management of malaria strategy is a WHO tool that identifies high risks groups such as children and pregnant women and prescribes pre-packed anti-malarial drugs for the treatment of fevers at home using community drug distributors. • This strategy has been successfully tested in rural areas but evidence remains low on how this strategy could be used in settings adopting expensive antimalarial combination strategies in rural areas where the CHW is the first point of contact.
Objectives • Main aim: • To assess the use of rapid diagnostic tests (RDTs) and ACTs for home management of simple malaria in children under five years old in Zambia. • Specific objectives: • To evaluate the clinical outcome of children under the age of five years treated with AL after RDT diagnosis of malaria at community level. • To asses the ability of a CHW to appropriately prescribe AL to children under five years old.
Planned analysis • Modeling • Relationship between malaria positivity and the variables for age/age group, sex, other complaints, region and fever • Will employ the logistic regression model, with the dependent variables as.factor
Results(1) • For the period under study, of the 2198 cases seen by CHWs, 67.0% were positive for malaria • 989 males (45.4%) who presented themselves with fever or other complaints • vs. 1188 females (54.6%). • However, in terms of proportions of positive malaria cases, • males had a slightly higher positive rate of 68.9% (95% CI, 66.0-72.0%) • Vs. female counterparts with 66.6% (95% CI, 63.9-69.3%).
Results(2) • In terms of rural versus peri-urban distribution of proportion of malaria cases, there was a significant difference, with the peri-urban site having 58.% of positive cases compared to 73.6% in rural site (t-test, p =<0.00001).
Results(3) • In line with adherence to the guidelines of treating only positive malaria cases diagnosed with RDT, the CHWs followed the instructions in 98.5% (1451) of cases (those who were positive and were treated with Coartem and only 1.5% of those who were positive did not receive treatment. • It was also noted that, 36.9% of negative RDT malaria cases received treatment >table(rdtresult,Treatment) Treatment rdtresult 1 2 0 261 446 1 1451 22
Results(4) • Sensitivity: for the CHWs adhering to the instructions, the probability to give treatment to a truly positive malaria case: Se = 1451/(1451+22) = 0.985 or 98.5% • Specificity: the probability not to give treatment to a negative malaria patient: Sp = 446/(261+446) = 0.631 or 63.1% • Predictive value of a positive test result: probability that treatment given corresponds to a truly malaria positive case VP+ = 1451/ (1451+261) = 0.847 or 84.7% • Predictive value of a negative result: probability in our situation that treatment not given corresponds to a truly malaria negative case VP- = 446/ (22+446) = 0.953 or 95.3%
Univariate analysis(using logistic regression) • Odds for the patient living in the rural area compared to those living in peri-urban areas for having a positive malaria test with RDT was 3.28 • Odds for a patient with fever to those presenting without fever was 2.34; • Odds for a patient younger by a year was 1.02 • Odds for patients presenting with other complaints compared to those with fever only was 0.44
Multivariate analysis • Starting with a saturated model, with the RDT result variable as a dependent variable and considering the variables for region, age, presence of fever at presenting, and complaints of other symptoms as independent variables. • As such the model was expressing the relation between the RDT result and age, region, presence of fever and other complaints in terms of risk (or probability).
Interpretation of final model • The log odds and probability to test malaria positive with RDT for a older patient from rural area presenting with fever is: • Ln(p/(1-p)) = 0.700 + 0.594 – 0.013 + 0.295 = 1.576 • Therefore, the probability to test malaria positive with RDT for a younger patient from rural area presenting with fever is = 0.830
Conclusion • CHWs were capable of appropriately prescribing Coartem based on RDT test results as reflected by the PPV (84.7%) and the NPV (95.3%) • Use of RDT and Coartem at community level further reduce the workload for the Health centres • Use of RDT and Coartem was highly acceptable by the community • Triggered further research for Cost Effectiveness Assessment
Acknowledgement Acknowledgement The funding was made possible from the World Bank through the Ministry of Health, Zambia. To all the participants in the communities in which we carried this study To the CHWs for their commitment and support of the project Health facility workers and DHMT staff for supervising role. Ministry of health for ensuring support and timely release of funds QRA Class 2009, particularly, Prof Speybroeck