HIV Management 2011
950 likes | 1.2k Views
HIV Management 2011. John K. Midturi April 16, 2011. Objectives. Recognize HIV/AIDS prevalence rates in USA Recognize populations at highest risk for HIV infections Understand rationale for CDC recommendations on routine testing Be able to decide when to initiate HAART

HIV Management 2011
E N D
Presentation Transcript
HIV Management 2011 John K. Midturi April 16, 2011
Objectives • Recognize HIV/AIDS prevalence rates in USA • Recognize populations at highest risk for HIV infections • Understand rationale for CDC recommendations on routine testing • Be able to decide when to initiate HAART • Be able to select initial antiretroviral regimen
Epidemiology • Reported 25 yrs ago • Industrialized nations • Chronic manageable disease • Developing world • Devastating effects on individuals, family units, general community • High mortality and morbidity rates
Estimated Incidence of AIDS, Deaths, and Prevalence by Quarter-Year of Diagnosis/Death, United States, 1985-1999* 25,000 350,000 1993 definition AIDS implementation Deaths 300,000 Prevalence 20,000 250,000 15,000 200,000 Number of Cases/Deaths Prevalence 150,000 10,000 100,000 5,000 50,000 0 0 1985 1986 1987 1988 1989 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 Quarter-Year *Adjusted for reporting delays
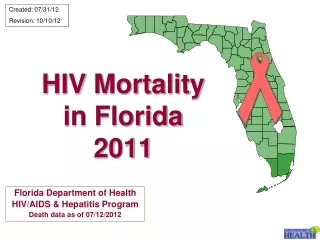
Estimated Rates for Adults and Adolescents Living With HIV Infection (not AIDS) 34 States and 5 U.S. Dependent Areas, 2007 American Samoa NorthernMarianaIslands Guam DC Estimated HIV Rateper 100,000 Confidential name-basedHIV infection reporting not implemented as of 2003 2.2 – 51.7 AK HI 51.8 – 103.8 103.9 – 170.5 Puerto Rico 170.6 – 282.0 Note: Rates have been adjusted for reporting delays. Inset maps not to scale. HIV/AIDS Surveillance Report, 2007. Vol 19, table 11. Data classed using quartiles Total rate: 154.2 per 100,000 U.S. Virgin Islands 6
Awareness of HIV Status in the US • From 2004 to 2007, the estimated number of newly diagnosed HIV/AIDS cases increased 15%3 1CDC. HIV prevalence estimate—United States, 2006. MMWR. 2008;57(39):1073-1076. 2Hall HI, et al. Estimation of HIV incidence in the United States of America. JAMA. 2008;300:520-529. 3CDC. HIV/AIDS surveillance report—cases of HIV infection and AIDS in the United States and dependent areas, 2007;19.http://www.cdc.gov/hiv/topics/surveillance/resources/reports/2007report/default.htm. Accessed July 23, 2009. 7
US Population Demographics: Total Population and HIV/AIDS Cases by Race/Ethnicity Total US Population (2006) (N = 247.1 million)1 Estimated HIV/AIDS Prevalence by Race/Ethnicity (2006)(N = 1,106,400)2 Other<2% Other 4% Hispanic/Latino18% White 71% Black 12% Black46% White35% Hispanic 13% Campsmith M, Rhodes P, Hall HI. 16th CROI; 2009; Montreal. Abstract #1036. 8
Estimated HIV/AIDS Prevalence and New Infections by Transmission Category in the US (2006) Estimated Prevalence of HIV/AIDS Estimated New HIV Diagnoses Other1% High-Risk Heterosexual Contact (Male)9% MSM + IDU4% MSM + IDU5% IDU (Female)7% IDU12% IDU (Male)12% High-Risk Heterosexual Contact31% MSM53% MSM48% High-Risk Heterosexual Contact (Female)18% CDC. HIV Incidence. Available at http://www.cdc.gov/hiv/topics/surveillance/incidence.htm. 9
A global view of HIV infection 33 million people [30–36 million] living with HIV, 2007
Pathophysiology and Natural History • Family of Retroviruses • Subfamilies • Oncoviruses • Lentiviruses- slow viruses • HIV- long replication periods prior to clinical manifestations • Spumaviruses- not associated with human disease
HIV genome consists of three structural genes • gag- codes for viral capsid proteins, p15, p17, p24 • pol- codes for proteins responsible for viral replication, and reverse transciptase • env- codes for envelope proteins gp120, gp41
Ontogeny of HIV • Simian immunodeficiency virus (SIV) is evolutionarily adapted to its natural hosts, chimpanzees and sooty mangeby monkeys • Inoculation of SIV into other primates typically produces an HIV-like disease • SIV is the closest known relative of HIV-1 and 2 • These findings suggest that the HIV pandemic began with infection of humans by SIV variants • Phylogenetic analysis suggests that HIV became established in humans early in the 20th century
HIV Types 1 and 2 • Geographic distribution • HIV-1: Global • HIV-2: West Africa • Transmission • Identical for the two virus types • Pathogenicity • HIV-2 appears to be less pathogenic than HIV-1
HIV-1 Classification System • Group M (main) • Subtypes (clades) A to D, F, G, H to K • Recombinant forms • Group O (outlier) • Group N (non-M/non-O)
HIV-1 Subtypes: Implications for Diagnosis and Treatment • Several studies suggest differential rates of HIV disease progression and transmission by subtype • There may be differential rates of emergence of resistance to ARVs by subtype
Transmission Un.org • Probability of infection • Blood transfusion/ transplant 95%-100% • MTCT with ART: ~25% • Needle Sharing: 1/150, ~0.6% • Occupational needle stick, 1/300, ~0.3% • Sexual contact (single event): 0.2% Medipulse.com Brandonyeoh.com
HIV Life Cycle 2. Membranefusion & entry Maturation 3. Uncoating & reverse transcription 7. Nuclearexport 1. Receptorbinding 8. Translation& Assembly 6. Transcription & RNA processing 9. Budding 4. Nuclearuptake 5. Integration
Immunopathogenesis of HIV • CD4+ cells are the principle targets of HIV in the host • Helper/inducer T-lymphocytes • Fetal thymocytes • Macrophages/monocytes • Dendritic cells • Microglia • Placental trophoblast cells
Acute infection • 40-90% of primary infections develop mononucleosis like syndrome • 2-6 weeks after exposure • Acute retroviral syndrome • Signs/symptoms • Fever 96%, LAD 74%, Exudative pharyngitis 70%, myalgia's/arthralgia 54%, diarrhea 32%, headache 32% • Duration of illness is <2weeks • Diagnosis • HIV RNA viral load (high) and HIV antibody (+/-)
Chronic Infection • Progressive loss of CD4 lymphocytes • 50-80 CD4 cells/uL per year • Infection to development of AIDS- 6-8years • Dependent on viral load, CD4 count, age, socioeconomic status, host genetics • Rapid progressor • Long term non-progressors • Elite controllers (viral load <48copies w/o therapy)
Definitions for AIDS Wikimedia.com www.bmj.com Emedicine.com www.brown.edu 1993 Centers for Disease Control and Prevention Revised Surveillance Definitions of AIDS
Screening and Diagnosis • CDC recommendations • 13-64 years of age • Routine HIV testing in all health care settings • Informed to opt out, no written consent required • Must screen for HIV • TB treatment • STD treatment • High risk behavior • IV drug users • Exchange sex for money • Sex partners of HIV infected person • Men who have sex with men • Heterosexual persons or partners with more than one partner since last test www.stdexpress.com
Routine HIV Testing: Who to Test Which patients should be offered routine HIV testing? What guidelines and recommendations exist regarding routine HIV testing? Short answer: All individuals between the ages of 13 and 64 yrs should be routinely screened for HIV infection in healthcare settings.
CDC Recommendations for Routine HIV Testing • Routine, voluntary HIV screening in healthcare settings recommended for all patients 13-64 yrs of age • Except in populations with documented prevalence of undiagnosed HIV infection < 0.1% • Without prevalence data, voluntary HIV screening appropriate until diagnostic yield < 1/1000 patients screened is established • Separate written consent not recommended • Pre- or post-test prevention counseling should not be required with testing or screening programs Branson BM, et al. MMWR Recomm Rep. 2006;55:1-17.
USPSTF HIV Testing Recommendations • Screening strongly recommended for all adolescents and adults at increased risk for HIV and all pregnant women USPSTF recommendations. July 2005.
Diagnosis • Enzyme linked immunosorbent assay (ELISA) followed by confirmatory Western blot assay if ELISA positive • ELISA 99% specific, 98.5% sensitive • Western blot 100% sensitive, and 100% specific for chronically infected • Detects antibodies to HIV proteins • Core (p17, p24, p55) • Polymerase (p31, p51, p66) • Envelope (gp41, gp120, gp160) Oraquick
Western Blot • CDC criteria 1 • p160, p120 AND p41 • CDC criteria 2 • p160, p120 OR p41 PLUS p24 • Positive= reactive to gp120 and either gp41, p24 • Negative= non reactive • Indeterminate= presence of other band pattern not positive • p160 • p120 • p41 • p68 • p53 • p32 • p55 • p40 • p24 • p18 GAG POL ENV
Diagnosis • HIV antibodies appear in circulation 2-12 weeks after exposure • Window period- serologic testing is negative • Repeat test in 6 weeks to 3 months • Rapid serologic tests results in 20 minutes • Sensitivity and specificity 99%
Management • H&P • Social support system • Reaction to HIV infection • Anxiety, depression, adjustment disorders • Lab • Baseline- assessment of liver, bone marrow, and kidney function, lipids • Cd4, viral load, CBC with diff, LFTs, lipid, hep Bs antigen and antibody, hep c antibody, Toxoplas IgG, cmv IgG, tst, rpr, pap smear, g6pd level, genotype
Preventative measures • Routine immunizations • Cervical cancer screening • Medication for primary or secondary prophylaxis
Immunizations • Pneumococcal vaccine • Every 5 years x 2 doses • Hepatitis A and B • Give when CD4 above 200cell/uL • TST/T-Spot • Annually • >5mm considered positive • CXR and if no symptoms and CXR clear therapy for LTBI
Women & HIV • Women • Increased incidence of cervical dysplasia and invasive cervical carcinoma • More frequent Pap smear screenings • 2 Pap smears 6 months apart and then annually if results are normal • Abnormality- colposcopy • HSV- suppressive therapy indicated for frequent anogenital outbreaks Kasheun.com
Care of Pregnant HIV-Infected Women The current recommendations focus on use of HAART by known HIV-infected pregnant women, regardless of maternal health needs reduce the risk of mother-to-child transmission Perinatal transmission rates—to less than 2%—in the United States. Identifying HIV infection in pregnant women with previously undiagnosed or newly acquired HIV infections Preventing HIV transmission to infants through the use of chemoprophylaxis antiretroviral therapy Avoiding breastfeeding http://www.hiv.gov.gy/ads/pstr_protectbaby.jpg
Antiretroviral Therapy During Pregnancy HAART should be initiated in all HIV-infected pregnant women regardless of CD4+ cell count or HIV-1 RNA level. Antiretroviral resistance testing before initiating HAART CBC & CMP testing before treatment initiation. OI prophylaxis-based on current CD4+ cell count. HAART (2 NRTIs and either a PI with ritonavir boosting or a NNRTI) Efficacy of antiretroviral therapy in preventing maternal to fetal transmission is primarily through lowering plasma HIV-1 RNA. Transmission can occur at any plasma HIV-1 RNA level, including undetectable plasma HIV-1 RNA All HIV-infected pregnant women should be offered HAART.
HIV-1 RNA Transmission % N 0/57 32/193 39/183 17/54 26/64 <1000 copies/mL 1000 - 10,000 10,001- 50,000 50,001-100,000 >100,000 0 16.6 21.3 30.9 40.6 Viral Load and Transmission Women & Infants Transmission Study (WITS) Garcia, et al, NEJM 1999
Mode of Delivery HIV-1 RNA remains > 1000 copies/mL- caesarian section Scheduled for 38-39 weeks gestation Intravenous zidovudine infusion initiated 4 hours before the caesarian delivery (2 mg/kg over 1-hour loading dose, then 1 mg/kg/hour continuous infusion until delivery, ie, umbilical cord ligated) Caesarian section delivery probably confers little added benefit in women with plasma HIV-1 RNA < 1000 copies/mL (Management Guidelines).[DHHS Perinatal] HIV-1 RNA is < 1000 copies/mL, a vaginal delivery Induction of labor at 38-39 weeks. Invasive fetal monitoring or operative delivery with vacuum devices or forceps should be avoided in HIV-infected women increase risk of transmission.[Mofenson 1999; Shapiro 1999] Artificial or prolonged rupture of membranes should be avoided caesarian delivery if labor does not progress 4 hours after membranes have ruptured Intravenous infusion with zidovudine should be initiated at the onset of labor Intravenous zidovudine (2 mg/kg over 1-hour loading dose, then 1 mg/kg/hour continuous infusion until delivery, ie, umbilical cord ligated)
Prophylaxis • CD4 cell count is an indicator of immune competence • CD4 <200, CD4% <14%, recurrent candidiasis, persistent fever, previous PCP: Pneumocystis jirovecii pneumonia • TMP/SMX • Dapsone • Atovaquone • Pentamidine (aerosolized)
Prophylaxis • CD4 <100 and positive IgG Toxo titer: • Toxoplasmosis: • TMP/SMX • Dapsone • Pyrimethamine • Leucovorin • CD4 <50 • MAC • Azithromycin • Clarithromycin • Rifabutin
Discontinuation of Prophylaxis • Discontinue primary and secondary prophylaxis for certain OI if sustained rise in CD4 cell count above threshold for prophylaxis initiation • PJP (>200) • Toxoplasmosis (>100) • MAC (>50) • Secondary prophylaxis • Cytomegalovirus (>150) • Re-initiate prophylaxis if CD4 decreased below threshold
Treatment • Goal: • prolong life • avoid destruction of immune system • allow reconstitution of immune system • prevent OI • provide improved quality of life by reduction HIV-related symptoms • Effective therapy: <50copies/ml • Improve prognosis, minimize the development of resistance, and prolong duration of antiretroviral response www.abc.net.au