Lymphoid Neoplasms
330 likes | 482 Views
What are the different types of lymphomas? What are the clinical manifestations and consequences? What to do if you suspect lymphoma as a differential dx ?. Lymphoid Neoplasms. Lymphocytic Leukemia

Lymphoid Neoplasms
E N D
Presentation Transcript
What are the different types of lymphomas?What are the clinical manifestations and consequences?What to do if you suspect lymphoma as a differential dx?
Lymphoid Neoplasms Lymphocytic Leukemia Neoplasm associated with widespread involvement of marrow, accompanied by large numbers of tumour cells in peripheral blood. Lymphoma Neoplastic tissue masses arising as discrete tissue masses.
Just note- These similarities have led to the grouping of some lymphomas and leukemias together as they share features: • Chronic lymphocytic leukemia and small lymphocytic lymphoma • Precursor B cell lymphoblastic leukemia and pre-B Cell lymphoblastic lymphoma • Pre-T cell lymphoblastic leukemia and pre-T cell lymphoblastic lymphoma
Lymphoma • Hodgkin Lymphoma • Reed Steenbergcells • (B cell origin) • Non – Hodgkin Lymphoma • Precursor B cell Neoplasm • Peripheral B cell Neoplasm • Precursor T cell neoplasm • Peripheral T cell and NK neoplasm 85% of lymphoid neoplasms are of B cell origin. Remainder being T cells. Occasionally they are NK cells. Further classification is done as: Indolent years), Aggressive (months), Highly Aggressive (weeks), Hodgkin (good prognosis)
Precursor B and T cell neoplasms (highly aggressive) • Hodgkin or non hodgkin? • Precursor B cell neoplasms arise in the bone marrow. Resulting in Leukemias. Precursor B cell Acute lymphoblastic leukemia. • Precursor T cell Neoplasms can arise in either the bone marrow or the thymus. Therefore developing either Precursor T cell Acute lymphoblastic leukemia/lymphoma.
Mature B cell neoplasms These tumors can be derived from any stage of mature B cell development, including naive B cells, germinal center B cells, post-germinal center memory B cells, or plasma cells. The most common B cell neoplasms derive from cells that have experienced a germinal center reaction.
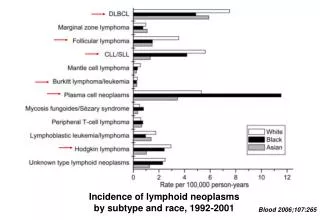
Chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL) — CLL/SLL is the most common leukemia in Western countries. small, mature-appearing lymphocytes, presenting primarily either as a leukemia (CLL) or a lymphoma (SLL). • Lymphoplasmacytic lymphoma (LPL) — LPL is a neoplasm derived from post-germinal center B cells • Mantle cell lymphoma (MCL) • B-cell prolymphocyticleukemia (B-PLL) • Follicular lymphoma (FL) — FL, previously called follicle center lymphoma, is the second most common lymphoma in the United States and Western Europe. • Diffuse large B-cell lymphoma (different sub types) • Burkitt lymphoma/leukemia • Marginal zone B-cell lymphoma (MZL) • Hairy cell leukemia (HCL) • Plasma cell myeloma/plasmacytoma • AL (primary) amyloidosis and light and heavy chain deposition diseases
Mature T-cell/Nkneoplasms • List equally as long as for B cell • Most common is peripheral T cell lymphoma (PTCL). This accounts for 15% of NHL. • Can have neoplasm of both myeloid and lymphoid origin.
Hodgkin Lymphoma • Arises from germinal center or post-germinal center B cells. HL has a unique cellular composition, containing a minority of neoplastic cells (these are the Reed-Sternberg cells and their variants) within an inflammatory background. • Divided into two sub-groups, based on appearance and immunophenotype of the tumorcells. These are • Nodular lymphocyte predominant HL (non classical) — The tumor cells in this subtype retain the immunophenotypic features of germinal center B cells. (variant of RS cell) Non classical hodgkins lymphoma only comprises 5% of cases • Classical HL — The tumor cells in this group are also derived from germinal center B cells, but typically fail to express many of the genes and gene products that define normal germinal center B cells. Based on differences in the appearance of the tumor cells and the composition of the reactive background, it is sub divided again: 1)Nodular sclerosis classical HL (most common) 2)Mixed cellularity classical HL 3)Lymphocyte-rich classical HL 4)Lymphocyte depleted classical HL
Clinical presentation of NHL • Presentation differs greatly (type/location) • Aggressive tumours present with a rapidly growing mass and systemic B symptoms (fever >38, night sweats, weight loss) • Indolent lymphomas present with slow growing lymphadenopathy, hepatomegaly, splenomegaly, or cytopenias. • Less common presentations, most frequently seen with T cell lymphomas, include skin rash, generalized fatigue, malaise, fever of unknown origin, ascites, effusions. • Patients with primary gastrointestinal (GI) tract lymphoma -anorexia, weight loss, nausea and vomiting, chronic pain, abdominal fullness, early satiety, visceral obstruction, acute perforation and GI hemorrhage
CNS lymphoma may present with headache, lethargy, focal neurologic symptoms, seizures, paralysis, spinal cord compression • Complications from tumourare many and varied, these may be the presenting problem. • Interesting point: Acquired angioedema (AAE) can occur (swelling and skin rash). This may be due to mass activation of the complement cascade and a resulting depletion of C1 inh protein. Or Neoplastic B cells producing autoantibody against it. C1 inh protein regulates bradykinin.
Spinal cord compression • Pericardial tamponade • Hypercalcemia (eg, adult T cell leukemia-lymphoma) • Superior or inferior vena cava obstruction • Hyperleukocytosis (eg, B or T cell lymphoblastic leukemia/lymphoma) • Acute airway obstruction (eg, mediastinal lymphoma) • Lymphomatous meningitis and/or CNS mass lesions • Hyperuricemia and tumorlysis syndrome • Hyperviscosity syndrome (eg, lymphoplasmacytic lymphoma with Waldenstrommacroglobulinemia) • Intestinal obstruction, intussusception • Ureteral obstruction, unilateral or bilateral hydronephrosis • Severe hepatic dysfunction • Venous thromboembolic disease • Severe autoimmune hemolyticanemia and/or thrombocytopenia (eg, small lymphocytic lymphoma)
Rarely may present with abnormal findings on lab results; hypercalceamia, hyperuriceamia, Increased LDH, serum protein electrophoresis. • Paraneoplastic syndromes.
A Tribute To the almighty Paul Conway Who defeated me on the obstacle course I humbly accept defeat
History • Family history of lymphomas • Exposure to cetain agricultural pesticides, toxins implicated in NHL • Relevant infections (HIV/EBV/HCV) • Immunodeficiency disorders • Inflammatory Gidiseases, H.pylori infection (crohns)
Presenting Complaints • Systemic B symptoms in 40%. More common in aggressive disease. • Lymphadenopathy- >2/3of patients with NHL present with peripheral lymphadenopathy. (ask about history of lump). Exclude infection. • Fever of unknown origin
Physical examination • Lymphoid survey (Waldeyers, liver/spleen, abdominal nodal sites, regularly palpable nodes). • Chest and lungs- 20% of patients with NHL present with mediastinaladenopathy on chest radiograph. This may be asymptomatic or cause cough, chest discomfort. • Superior vena cava syndrome as a result of compression (3-8%) • Chylopericardium, chylothorax, chylousascites can be present if major obstruction to thoracic duct.
50% of patients will develop extranodal disease. Most common site site is GI tract followed by skin.
Hodgkin lymphoma • Bimodal age distribution, peaks 20-30, then again over 50. • Most patients present with overt disease, most commonly asymptomatic enlarged lymph node or mass on chest xray. • Symptoms non specific and more compatible with infection (B symptoms). Fever more noticeable in evening. Pruritis • Asymptomatic lymphadenopathy in 70%. Non tender and rubbery. Spreads to adjacent nodes rather than haphazardly. • Retro lymphadenopathy may give rise to loin pain. • Alcohol induced pain (within a few minutes)
Burkitts lymphoma • Endemic (african), • non endemic (sporadic) 30% of pediatric lymphomas, • immunodeficiency related.
Staging is not necessarily prognostic • Measures locations • Not actual tumour burden • Histology and clinical parameters are better indicators • International prognostic indicator (IPI)
Patients with generalized lymphadenopathy should have a CBC and chest x-ray. If these are normal, other considerations include a PPD (TB), HIV antibody determination, RPR (syphilis?), ANA (Autoimmune), and heterophile (EBV). • Patients with localized lymphadenopathy can be observed for three to four weeks if there is nothing else in the history and physical examination to suggest malignancy. • This approach is safe and avoids unnecessary biopsies since the adenopathy will resolve or the cause will become obvious in many patients during that time. Diagnostic tool of time? “Even with "can't miss" diagnoses such as Hodgkin lymphoma, head and neck cancer, or tuberculosis, the window of opportunity for effective treatment is likely to remain open during this period of observation.” Biopsy is appropriate if an abnormal node has not resolved after 4/52, perform immediately in patients with other findings suggesting malignancy. Empiric treatment of unexplained lymphadenopathy with antibiotics is not useful.
LYMPH NODE AND TISSUE BIOPSY A biopsy is required for the diagnosis and classification of NHL. This should be obtained urgently if an aggressive NHL is suspected. Lymph node selection — The decision to biopsy a lymph node is dependent upon the clinical situation, characteristics of the patient (age, gender) and location. Regardless of whether lymphadenopathy is localized, regional, or generalized, if other diagnostic tests do not support another diagnosis, a lymph node should be considered for biopsy if 1 or more present: -Significant enlargement (>2.25cm²) -Persistence for more than four to six weeks -Progressive increase in size
Type of biopsy — Most patients presenting with enlarged lymph nodes have a benign form of reactive lymphadenopathy. Fine needle aspiration (FNA) as an initial screening test. When coupled with comprehensive immunophenotyping (typically flow cytometry), FNA is particularly useful at distinguishing reactive B cell hyperplasias from clonal mature B cell neoplasms. However, the general consensus is that accurate histopathologic evaluation requires a tissue biopsy, preferably an intact lymph node, FNAs suggesting the presence of a lymphoma definitive tissue biopsy