Download

1 / 20
200 likes | 399 Views
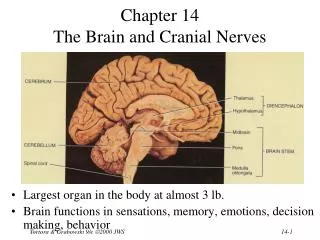
Tony Figaji MBChB, MMed, FCS, PhD Head of Pediatric Neurosurgery Red Cross Children’s Hospital University of Cape Town. Monitoring the brain: What’s worthwhile?. Everything. Neurocritical care is underdeveloped Pediatric neurocritical care is even worse

E N D
Tony Figaji MBChB, MMed, FCS, PhD Head of Pediatric Neurosurgery Red Cross Children’s Hospital University of Cape Town Monitoring the brain:What’s worthwhile?
Everything Neurocritical care is underdeveloped Pediatric neurocritical care is even worse Secondary brain injury is underappreciated
Challenges The brain is complex Children are physiologically different Individual and temporal heterogeneity Many different causes for raised ICP, standard Rx Surrogate markers of brain health used Direct measures of brain physiology?
Practical technology in the ICU - options • Brain tissue oxygen tension • Near-infrared spectroscopy • Jugular venous saturation • Continuous EEG • Microdialysis • TCD / autoregulation • Continuous CBF • Physiological imaging
Why is ICP monitoring not good enough? • Classic cellular oedema • Hyperemia • Vasospasm • Subclinical seizures • Impaired autoregulation GCS 4 ICP = 35 BrO2 low CBF↓/N BrO2 high, FV / CBF high GCS 4 ICP = 35 GCS 4 ICP = 35 BrO2 low, FV high/ LR↑ GCS 4 ICP = 35 BrO2 low, EEG typical GCS 4 ICP = 35 BrO2 passive, ARI low
Low BrO2 is associated with poor outcome Examined associations with outcome in multivariate model: clinical, physiological, radiological Adjusted Odds Ratio for poor outcome: PbtO2<10 for >2 hours OR 10.8 (1.4-82.4) PbtO2<5 for >1 hour OR 27.4 (1.9-391) Strongest independent predictor of outcome Mortality for series = 9.6% Childs Nerv Syst. 2009 Oct;25(10):1325-3
It is not predicted by measures of initial injury severity It is not a surrogate marker of something else
Brain hypoxia/ischemia is common despite observing current thresholds for treatment based on available evidence % of pts Figaji et al, Neurosurgery. 2008 Jul;63(1):83-91
It has a complex relationship with ICP ? BrO2 ICP
N=75 children 9452 hrs monitoring
ICP PbtO2 MAP
Can evaluate the effects of intervention BrO2 decompressive craniectomy Figaji et al, Acta Neurochir Suppl. 2008;102:77-80
Increase in blood pressure ICP PbtO2 MAP ICM+ Pressure autoregulation, intracranial pressure and brain tissue oxygenation in children with severe traumatic brain injury Figaji et al. J Neurosurg Peds, 2009;4:420-8
Blood transfusion Baseline values 4 hour period post-RBCT PbtO2 : 28.7 ± 6.8 mmHg CPP : 64 ± 15 mmHg FiO2 : 46 ± 12% PbtO2 : 33.3 ± 11.8 mmHg CPP : 70 ± 13 mmHg FiO2 : 47 ± 13% P=0.002 P=0.021 P= 0.474 Account for CPP change: Co-efficient 0.3356, P=0.001 The effect of blood transfusion on brain oxygenation in children with severe traumatic brain injury Figaji et al. Pediatric Crit Care Med 2009
Increase in PaO2 ↓FiO2 ↑FiO2 PbtO2 ICP
Patients are different • 34 patients, 291 TCD studies • Mean Flow Velocity (MCA): 95 (79-115) range 32-180cm/s Figaji et al, Surgical Neurology 2009; 72:389-394
Will monitoring make my patients better? • Gives us more information • Lets us know when patients are getting into trouble before an established problem • Helps interpret the underlying pathophysiological problem • Helps us titrate therapy appropriately • Probably reduces secondary injury • Yes • No • Depends on correct application and interpretation • Intervention misapplied can have equally hazardous effects • The treatment may be worse than the problem
Summary ‘Monitors alone cannot save a patient, but wise application of the data from monitoring the injured brain can’ Saul and Ducker, 1982