CCCHAP-MN HepatitIs Update
170 likes | 392 Views
CCCHAP-MN HepatitIs Update . Presented by Cheri Booth, MPH MN Department of Health November 22, 2013. What is Hepatitis?. What is it caused by How is it spread Who is most affected What are the outcomes?. What causes hepatitis? . Hepatitis is basically inflammation of the liver.

CCCHAP-MN HepatitIs Update
E N D
Presentation Transcript
CCCHAP-MN HepatitIs Update Presented by Cheri Booth, MPH MN Department of Health November 22, 2013
What is Hepatitis? What is it caused by How is it spread Who is most affected What are the outcomes?
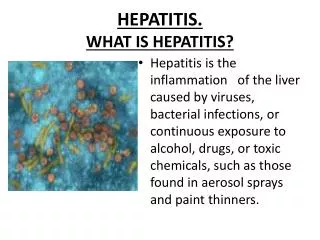
What causes hepatitis? • Hepatitis is basically inflammation of the liver. • (hepat-) = liver, (-itis) = inflammation • Many things can cause hepatitis: • Caused by viruses, alcohol, medications, and other toxins • Can also be caused by genetic conditions or co-morbidities
How is hepatitis spread • VIRAL hepatitis is spread from person to person or from the environment. Exactly how depends on which hepatitis virus. • Hepatitis A – food borne, and to a much smaller degree sexualor IDU • Hepatitis B- blood, sex, perinatal • Hepatitis C (has 24 different genotypes!) • Blood, and to a much smaller degree perinatal or sexual • Hepatitis D- ‘piggy back virus’- blood, sexual • Hepatitis E- same as type A • Hepatitis G- very similar to ‘C’
Who is most affected? • HBV- In MN it is primarily persons born in endemic areas who relocate here. Transmission often occurs at birth. Or in early adulthood by blood, sexual contact, or unsterilized/ contaminated medical supplies. • HCV- Approx5.5 million Americans infected. Highest prevalence is among ‘Baby Boomers’. • Related to blood exposures such as transfusion in the days before the virus was isolated as well as military exposures. • Most aren’t aware of status. • HCV- Greatest incidence is among persons who inject drugs. More often in <30’s. • Related to opioid addiction and injection use trends.
Outcomes • HBV- If infected at birth or in childhood outcome is nearly always chronic infection. Adults tend to clear the virus in 85% of infections. High rates of cirrhosis and liver cancer for chronically infected. • HCV- Majority of those infected become chronic cases (~70%). Greatest indicator for liver transplant in the US. Most with lifelong infection will develop some level of fibrosis and or cirrhosis. Liver cancer rates rising dramatically.
Hep C in MN How many Minnesotans are affected by HCV Which populations or locations are experiences higher burden of infection?
HCV Infected Persons Identified through Passive Surveillance in MN through 2012 N=84,863** 39,303 HCV infected persons* identified through passive surveillance Estimated unidentified HCV infected persons 45,559 *Includes all acute, chronic, probable chronic, and resolved cases. **http://www.cdc.gov/ncidod/diseases/hepatitis/c/fact.htm Data Source: MN Viral Hepatitis Surveillance System
Persons Living with HCV in MN by Age, 2012 Median Age: 55 Data Source: MN Viral Hepatitis Surveillance System
Persons Living HCV in MN by Gender*, 2012 *Includes anonymous methadone patients Data Source: MN Viral Hepatitis Surveillance System
Persons Living with Chronic HCV in Minnesota by Race, 2012 Afr Amer = African American /Black Asian=Asian or Pacific Islander Amer Ind = American Indian Other = Multi-racial persons or persons with other race
Persons Living with HCV In MN Rates (per 100,000 persons*), 2012 *Rates calculated using 2010 U.S. Census data Excludes persons with multiple races or unknown race Data Source: MN Viral Hepatitis Surveillance System
Trends in Hepatitis C in the US • Young (under 30) people have had a significant increase in rate of HCV infection. • Future implications related to morbidity and mortality, perinatal transmission of HCV, and treatment costs. • Opioid addiction and heroin purity in MN leading to greater issues of addiction, unsafe injection behavior, and overdose.
Increasing Morbidity and Mortality Related to Hepatitis C • HCV is a major cause of liver disease • Leading indication for liver transplantation • Leading cause of hepatocellular carcinoma (HCC) (approx.50% of HCC incidence) • Over the next 40-50 years, a projected: • 1.76 million with untreated HCV infection will develop cirrhosis • 400,000 will develop HCC • 1 million will dies from HCV-related complications • Substantial HCV-related costs1 • Exceeds $5 billion annually • 2010-2019 estimated costs total $54.2 billion 1 McGarry et al. “Economic Model of a Birth Cohort Screening program for Hepatitis C” Hepatology 2012; 55:1344-1355
Taking Action The role of community planning/ HIV advisory committees in the fight against viral hepatitis
HIV and HCv- if the shoe fits…. • Natural cross-over between populations affected and how prevention and linkage to care work is done. • Ability to enhance existing services rather than recreate them. PCSI opportunity! • Rapid HCV test allows alignment with current HIV testing strategies and programs • Advocacy/ provision of care around hepatitis C testing and referral often strengthens inroads into difficult to reach populations in need of HIV services.
Incorporation of Hepatitis • Many states have incorporated Hepatitis into their HIV community planning groups. • Logical fit based on population overlaps, funding goals, and federal imperative to incorporate/ collaborate services. • Challenging to operate even one advisory group. Adding a second would be a burden to communities already finding it difficult to participate. • Precedence and trend toward combining groups is seen across the nation. • CDC, NASTAD • NY, CA, MA, TX, CO, DE, VT, etc………………………..