Download
1 / 55
550 likes | 666 Views
Detailed case study of an elderly lady presenting with acute thoracic pain; history, investigations, differential diagnosis, and treatment plan explored thoroughly.

E N D
Something in the blood? By: Navdeep Brar, Andrew Shute, John Ong Student Grand Round Tuesday, 25 Nov 2003
PC • 11.11.2003 • Pleasant 78 yr old lady presenting in A&E with acute right thoracic pain radiating from back to anterior chest
HPC • Receiving treatment for recent pleural effusion (18.09.2003) • Dry, non-productive cough for 7/52; some SOB; ° haemoptysis; ° wheeze • Pain started early previous morning • Pain – sharp, sudden, constant; associated headache; ° N & V • Not relieved by paracetamol or posture; worse on deep inspiration • ° recent travel, immobility or leg pain
PMH • Recurrent admissions for similar complaints over last 4 years • 2 x previous PE (1992, 1999) • Subdural haematoma (1992) • 2 x TIAs (1994 & 2000) • Hiatus hernia; acute pancreatitis; diverticulitis • Scoliosis with back pain • ° JTHREADS; ° MI
PMH continued • Warfarinised after first PE in March 1992 • April 1992 presented with daily, constant headaches for 5/52; worse in mornings, when coughing and straining • CT showed bilateral subdural haematoma L > R; INR 2.7 • Warfarin stopped. • Started on aspirin 75mg od
PMH continued • June 1992: CT check up showed persistent R hemisphere, chronic subdural haematoma with mass effect and shift. • R frontal burrhole drainage at Atkinson Morley Hospital • Sept 1992 check up showed good progress
PSH • Cholecystectomy (2001) • Bilateral cataract removal (1990s) • Neurosurgical evacuation of sub-dural haematoma (1992) • Hysterectomy (1990)
MH • Omeprazole 40mg od • Aspirin 300mg od • Amoxycillin 500mg tds • Occasional paracetamol; ° herbal, complementary or recreational drugs • NKDA or side effects
GH • “Not as good as it used to be” though “previously quite healthy” • Lost some weight and mild anorexia since cough started • Sleeps well • No exercise but leads an active and busy life • Her back ache can stop her doing some activities
SH • Widowed for 18 years; 4 sons: 51, 46, 39 (non-identical twins) • Lives in 3 bedroom, terraced house with her youngest son • Has good family and home support • Enjoys reading and is active around the house • Retired though used to work as a typist, temp. and school help • ° smoking • occasional alcohol
FH • Father – glaucoma • Brother – died aged 56 from an embolism? • Brother – suffered from depression and died from an overdose?
Systems • CVS - right thoracic chest pain - ° palpitations, ° paroxysmal nocturnal dyspnoea, ° ankle swelling • Resp. - ° SOBOE - sleeps with 2 pillows • GI - often has constipation or diarrhoea - occasional heartburn • GU - mild nocturia • Neuro. - occasional migraine - numbness on her right hand (medial distribution) - prescription glasses, ° hearing problems • MSS - ° stiffness or pain in limbs - constant backache
O/E 11.11.2003 • Px c/o chest pain and headache; seems quite tired and ill • Pulse: 97, BP: 152/85, RR: 22, Temp: 37o,O2 sats: 96 air, • JVP 5 mm, HS I + II + 0 • o oedema, calf swelling or tenderness • Chest resonant • AE ↓ right base, right basal dullness • o masses or organomegaly
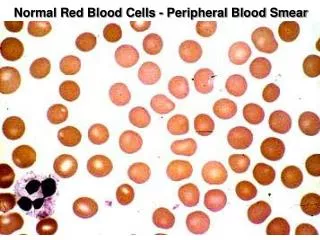
Investigations • FBC, D-dimers, Blood culture, U&Es, LFT, Bone Profile, glucose, CK, CRP, Trop T, ABG • ECG and CXR • Albumin 32 (35-48) • Sensitive CRP 99.1 (0-8) • Hb ↓ 11.3 (11.5-16) • ABG: PaO2 ↓ 8.62 (>10.6) • Gamma GT 43 (0-30) • D dimers ↑ 0.79 • ECG – sinus rhythm, RBBB, Qs III, • CXR – small right pleural effusion
Differential diagnosis • PE • Pleural effusion exacerbation • Other chest infection Plan: • Troponin T, thrombophilia screen, V/Q scan, ?CTPA • Co-dydramol 2 tabs oral • Voltrol 50 mg • Fragmin 10000 SC
Pulmonary Embolism • Most often due to venous thrombus in the abdomen, pelvis or legs • Part of a clot breaks off and passes through the heart before lodging in the pulmonary circulation • Ventilation is normal but perfusion is reduced
PE Risk Factors • Any cause of recent immobility or hypercoagulabiltiy: • recent surgery; stroke; MI • prolonged bed rest (E.g. infection) • Thrombophilia • Disseminated malignancy • Pregnancy, postpartum; The Pill/HRT • Advanced age
PE - clinical features • Depend on number, size and distribution of emboli: • Small - often asymptomatic • Large - often fatal • Acute breathlessness; pleuritic chest pain; haemoptysis; dizziness. • Pyrexia; cyanosis; tachypnoea; tachycardia; hypotension; raised JVP; pleural rub/effusion
Why PE? • Previous history • Advanced age • Immobility for last 7 weeks with cough • SOB; Pleuritic chest pain; raised JVP • Evidence of pleural effusion • Support from ECG and CXR • PaO2 ↓ 8.62; D dimers ↑ 0.79
12.11.2003 • ° SOB, ° headache, pain ↓, “feels well” • V/Q scan – unmatched perfusion defect in the right midzone anteriorly, but unchanged since previous scan on 09.01.2002. • This indicated that there was no evidence of a new PE
13.11.2003 • ABG - PaO2 11.71 kPa, PaCO2 4.83 kPa • Px feels much better 14.11.2003 • Px discharged – probable muscular pain as result of cough combined with underlying pleural effusion • Aspirin 300mg od, Ibuprofen 400mg prn, Paracetamol 1g prn • Results of thrombophilia screen to be sent to GP if abnormal
Warfarin Sodium • Anti-coagulant acts by inhibiting vitamin K dependent coagulation factors • Factors II, VII, IX, X & anti-coagulation proteins C & S • Racemic mixture of R + S enatiomers • S enatiomer has 2-5 times more anti-coagulant activity • Takes at least 48-72hrs for anti-coagulation effects to develop fully • Immediate effect Heparin must be given concomitantly
Pharmacokinetics • Absorption • completely absorbed after oral administration-peak concentration attained 1st 4hrs. • Distribution • No difference after I.V and oral administration • 0.14L/kg volume of distribution • Concentration in foetal plasma approach maternal values • 99% bound to plasma proteins
Pharmacokinetics • Metabolism • Eliminated almost entirely by metabolism-hepatic microsomal enzyme (cP450) & reductases. • Excretion • Excreted in urine & bile • Effective t1/2 = 20-60 hours • Elderly • No significant age-related difference in phamacokinetics of racemic warfarin • As age increases less warfarin is required to produce therapeutic levels of anti-coagulation
Phamacokinetics • Renal dysfunction • No dosage adjustment necessary for patients with renal failure • Hepatic dysfunction • can potentiate the response to warfarin- through impaired synthesis of clotting factors and decreased metabolism
Indications • Prophylaxis and/or treatment: • Deep venous thrombosis • Pulmonary Embolism • Atrial Fibrillation with risk of embolisation • Cardiac valve replacement to prevent emboli developing on these • Post Myocardial Infarction- reduce risk of death, recurrent MI, stroke & systemic embolisation.
Dosage & Administration • Individualised for each patient according to the particular patients prothrombin time, reported as international normalised ratio- INR. • INR is a value derived from a standardised laboratory test that measures the effect of an anticoagulant. • Normal blood has an INR 1. • Therapeuitc anti-coagulation aims to achieve an INR of between 2.0-3.5.
Dosage & Administration • DVT & PE • INR 2.0-3.0 is sufficient for prophylaxis and treatment • AF • Effects of warfarin in reducing thromboembolic events such as stroke were similar at high INR 2.0-4.5 or low INR 1.4-3.0. • Post M.I • Wafarin therapy should be initiated early (2-4 weeks post M.I) and adjust dosage to maintain INR of 2.5-3.5 long-term. • Cardiac valve replacement • Mechanical heart valves long term prophylaxis to an INR of 2.5-3.5. • Bioprothetic heart valves for warfarin therapy to an INR 2.0-3.0 for 12 weeks after insertion.
Dosage • InitialDosage • Varies for each Individual according to patient’s drug sensitivity • Large loading dose may increase risk haemorrhages & no evidence for increased protection against thrombi formation • Low doses recommended for elderly and/or debilitated patients • Maitenance • 2-10 mg daily • continued until the danger of thrombosis and embolism pass
Side Effects • Fatal or non-fatal haemorrhage from any tissue or organ • may present as paralysis, headache or pain in other areas, dizziness, shortness of breath, weakness, hypotension and unexplained shock. • Bleeding-occurs when PT/INR is within therapeutic range • may unmask a previously unsuspected lesion e.g tumour or ulcer. • Infrequent adverse reactions • These include Hypersensitivity reactions, systemic cholesterol microembolization, purple toes syndrome, vasculitis, hepatitis, cholestatic hepatic injury, jaundice,elevated liver enzymes.
Warnings • Narrow therapeutic index drug and maybe affected by factors such as other drugs and dietary vitamin K. • Administration of drugs in the following conditions need to considered in terms of risks of therapy weighed against benefits: • Lactation • Severe to moderate hepatic insufficiency • Infectious Diseases • Trauma • Surgery • Known or suspected Deficiency in Protein C mediated Anticoagulant Response • Polycythemia vera, vasculitis, severe diabetes
Definition • SDH is defined as “an accumulation of blood in the space between the dura and the dura mater following the rupture of a vein(s) running from the hemisphere to the sagittal sinus.” Epidemiology • 1/3 of all severe blunt head trauma (GSC < 9) in US (UK?) • Occurs in men > women
Dura reflected back to show bridging veins that drain from the cortex to sagital sinus. Dura reflected back to show a subdural haematoma.
Pathology • Rupture of veins within the dura leakage + accumulation of blood in subdural space • Commonly due to blunt head trauma and very rarely occurs spontaneously • Generally divided into 3 groups: Acute, Subacute, and Chornic
Pathology (Cont’d) • Acute - rapidly clotting blood collection 0-2 days of injury. Associated with high mortality (20%) and morbidity rates. • Subacute – clotting blood collection within 3-7 days of injury • Chronic – 2-3 weeks after injury • Note: Complicated SDHs are associated with 50% mortality rates. ( Rupture is assumned to occur at time of acute injury)
Signs • Raised ICP • Localized neurological symptoms • Shifted midline structures away from side of the clot (if clot is sizeable) • Tentorial herniation and Coning (may occur if untreated).
Symptoms • headache, drowsiness, confusion • Physical + Intellectual slowing, • sleepiness, • personality change • unsteadiness • symptoms fluctuate in about 35% of patients and may surface a few weeks to a few months after the injury
Risks Factors / People At Risk • Infants • adhesions in subdural space absent at birth and develop with age bilateral SDHs are more common in infants • Victims of child abuse • Associated with Inter-hemispheric SDH • Alcoholics • Prone to head trauma, thrombocytopenia, prolonged bleeding times
People At Risk (Cont’d) • Elderly • (accident prone, atrophic brains make connecting veins more susceptible to rupture) • Epileptics • Patients on Anti-coagulants • Haemophiliacs
Investigations • FBC • Coagulation Profile (INR, PT, aPTT) • Electrolytes • Type and screen/cross • CT • MRI (if CT is insufficient)
Diagnosis • Acute SDH • typically a hyperdense (white) crescentic mass • along the inner table of the skull, most commonly over the cerebral convexity in the parietal region.
Diagnosis (Cont’d) • Subacute Phase SDH • lesion becomes isodense (wrt brain) and is harder to see on a CT scan • MRI and contrast CT scan should be used Non-contrast CT scan MRI
Diagnosis (Cont’d) • Chronic Phase SDH • Lesion becomes hypodense and is easy to diagnose on normal CT scans Commonly bilateral, and have areas of acute bleeding, which result in heterogeneous densities
Differential Diagnosis • Stroke, • Cerebral tumour, • Dementia, • Subdural empyema, • Meningitis, • Subarachnoid haemorrhage, • Epidural haematoma, • Elderly and child abuse
Initial Management • Use GCS to ascertain level of consciouness (though it may fluctuate) • Consider Intubation if GCS < 12 or other conditions present that threaten airway/breathing. • Check for signs of focal neurological deficits & ICP • Recommended that any head trauma that results in a GCS <15 in a patient without the influence of any mind-altering or intoxicating substances, should require an urgent CT scan