Download
1 / 22
230 likes | 289 Views
Learn about Osteoarthritis (Degenerative Joint Disease, DJD) and Rheumatoid Arthritis (RA), their symptoms, management, and surgical interventions. Discover key strategies for pain relief, medication, therapy, and lifestyle adjustments.

E N D
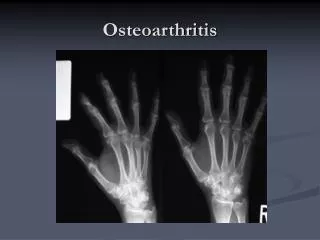
Osteoarthritis (Degenerative Joint Disease, DJD) • Progressive degeneration of the joints as a result of wear & tear. • Causes the formation of bony buidup & the loss of articular cartilage in peripheral & axial joints. • Affects the weight-bearing joints & joints that receive the greatest stress, such as the knees, toes, & lower spine. • The cause is unknown but may be trauma, fractures, infections, or obesity.
Osteoarthritis (Degenerative Joint Disease, DJD)- Assessment • Joint pain that early in the disease process diminishes after rest & intensifies after activity • As the disease progresses, pain occurs with slight motion or even at rest. • Symptoms are aggravated by temperature change & humidity. • Crepitus • Joint enlargement • Limited ROM • Difficulty getting up after prolonged setting • Skeletal muscle atrophy
Osteoarthritis (Degenerative Joint Disease, DJD) • Inability to perform activities of daily living • Compression of the spine as manifested by radiating pain, stiffness, & muscle spasm in one or both extremities. • Presence of Heberden’s nodes or Bouchard’s nodes
Osteoarthritis (Degenerative Joint Disease, DJD) Implementation • Administer NSAIDs, salicylates, and muscle relaxants • Prepare for corticosteroid injections into joints • Place affected joint in functional position • Immobilize the affected joint with splint or brace • Avoid large pillows under the head or knees • Provide a foot cradle • Position the client prone twice a day
Osteoarthritis (Degenerative Joint Disease, DJD) • Position the client prone twice a day • Instruct the important of moist heat, hot packs or compresses & paraffin dips • Apply cold applications when the joint is acutely inflamed. • Encourage adequate rest • Encourage a well-balanced diet • Encourage weight loss if necessary • Reinforce the exercise program & the important of participating in the program.
Osteoarthritis (Degenerative Joint Disease, DJD) • Instruct to stop exercise if pain is increased with exercising • Instruct to decrease the number of of repetitions in an exercise when the inflammation is severe. • Surgical Management: Osteotomy- the bone is cut to correct joint deformity & promote realignment. • Total joint replacement: performed when all measures of pain relief have failed. Hips & knees are most commonly replaced. Contraindicated in the presence of infection, advanced osteoporosis, or severe inflammation.
Rheumatoid Arthritis (RA) • Chronic systemic inflammatory disease; the etiology may be related to a combination of environmental & genetic factors. • Leads to destruction of connective tissue and synovial membrane within the joints. • Weakens & leads to dislocation of the joint & permanent deformity. • Exacerbations are increased by physical or emotional stress • Risk factors include exposure to infectious agents; fatigue & stress can exacerbate the condition.
Rheumatoid Arthritis (RA)implementation • Inflammation, tenderness, stiffness of the joints • Moderate to severe pain & AM stiffness lasting longer than 30 minutes • Joint deformities, muscle atrophy & decreased ROM • Spongy, soft feeling in the joints • Low-grade temperature, fatigue,& weakness • Anorexia, weight loss & anemia • Elevated ESR & positive RA • X-ray showing joint deterioration • Synovial tissue biopsy presents inflammation
Rheumatoid Arthritis (RA) • Pain-Salicylates (ASA). Monitor for side effects, including tinnitus, GI upset & prolonged bleeding time. Administer with meals or a snack. Monitor for abnormal bleeding or bruising. • Nonsteroidal antiinflammatory drugs (NSAIDS) May be prescribed in combination with salicylates if pain & inflammation have not decreased within 6 to 12 weeks following salicylate therapy. • Corticosteroids: Administer during exacerbations or when commonly used agents are ineffective.
Rheumatoid Arthritis (RA) • Antineoplastic medications: Administer in clients with life- threatening RA • Gold salts: Administer in combination with salicylates & NSAIDS to induce remission & decrease pain & inflammation. • Preserve joint function • Balance rest and activity • Prevent flexion contractures • Apply heat or cold therapy • Apply paraffin bath & massage
Rheumatoid Arthritis (RA) • Exercise only to the point of pain • Avoid weight bearing on inflamed joints • Identify factors that may contribute to fatigue • Monitor for signs of anemia • Administer iron, folic acid & Vitamin supplement • Monitor for drug-related blood loss by testing the stool for occult blood • Asses the client’s reaction to the body change • Encourage to verbalize feelings
Rheumatoid Arthritis (RA) • Surgical intervention: Synovectomy= removal of the synovia to help maintain joint function. • Arthrodesis: Bony fusion of a joint to regain some mobility. • Joint replacement (arthroplasty): removal of diseased joints with artificial joints; performed to restore motion to a joint & function to the muscles, ligaments & other soft tissue structures that control a joint.
Gout • A systemic disease in which urate crystal deposit in joints & other body tissues • Leads to abnormal amounts of uric acids in the body • Primary gouts results from a disorder of purine metabolism • Secondary gout involves excessive uric acid in the blood that is caused by another disease.
Gout (phases) • Asymptomatic: No symptoms. Serum uric acid is elevated. • Acute: Excruciating pain & inflammation of one or more small joints, especially the great toe. • Intermittent: Asymptomatic period between acute attacks • Chronic: results from repeated episodes of acute gout. Deposits of urate crystal under the skin and within the major organ, especially the renal system.
Gout (assessment) • Excruciating pain in the involved joints • Swelling & Inflammation of the joints • Tophi (hard, fairly large, & irregularly shaped deposits in the skin) that may break open & discharge a yellow gritty substance • Low-grade fever • Malaise & headache • Pruritis • Presence of renal stones • Elevated uric acid levels
Gout (implementation) • Provide a low purine diet • Instruct to avoid foods, such as organ meats, wines, aged cheese • Encourage a high fluid intake of 2000 ml to prevent stone formation • Encourage weight-reduction diet • Instruct the client to avoid alcohol 7 starvation diets because they may precipate a gout attack. • Provide bedrest during the attack
Gout • Monitor the joint in mild flexion during acute attack. • Elevate the affected extremity • Protect the affected joint from excessive movement or direct contact with sheets or blankets • Provide heat or cold for local treatments to affected joints • Administer NSAIDs & antigout medications.
Systemic Lupus Erythematosus (SLE) • A chronic progressive systemic inflammatory disease that can cause major organs & systems to fail. • Connective tissue & fibrin deposits in blood vessels, collagen fibers & organs • Leads to necrosis &/ or inflammation of blood vessels, lymph nodes, GI tract, pleura. • There is no cure for the disease. • Cause is unknown although the disease is due to defect in the immunological mechanisms or to have a genetic origin
Systemic Lupus Erythematosus (SLE) • Precipitating factors include medications, stress, genetic factors, sunlight or ultraviolet light & pregnancy. • Assessment: Dry scaly raised rash on the face or upper body • Fever, weakness, malaise, fatgue • Anorexia, weight loss, photosensitivity • Joint pain, erythema of the palms, anemia • Positive antinuclear (ANA) & LE prep. • Elevated ESR.
Systemic Lupus Erythematosus (SLE) (Implementation) • Monitor skin integrity & provide frequent oral care • Instruct to clean skin with mild soap, avoiding harsh & perfumed substances • Assist with the use of ointments & creams for rash • Instruct inmeasures to conserve energy, such as pacing activities & balancing rest with exercise.
Systemic Lupus Erythematosus (SLE) • Administer topical or systemic corticosteroids, salicylates & NSAIDs. • Administer hydroxychloroquine (Plaquenil) to decrease the inflammation. • Instruct to avoid exposure to sunlight & ultraviolet light • Monitor for proteinuria & red cell casts in the urine • Monitor for brusing, bleeding & injury.
Systemic Lupus Erythematosus (SLE) • Assist with plasmapheresis to remove autoantibodies & immune complexes from the blood before organ damage occurs. • Monitor for signs of organ involvement, such as pleuritis, nephritis, pericarditis, neuritis, anemia & peritonitis. • Provide supportive therapy as major organs become affected. • Provide emotional support & encourage to verbalize feelings. • Provide group information regarding support groups, & encourage utilization of community resources.