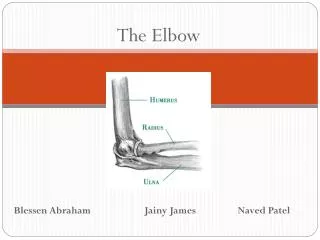
The Elbow
The Elbow. Ramy El Nakeeb, MD. Orthopaedic Department Damanhour Medical institute. Lateral Epicondylitis (tennis elbow ). Definition: “ Tendinopathy of the common extensor origin of the elbow” Pathology 30 – 50 years old Repetitive micro-trauma

The Elbow
E N D
Presentation Transcript
The Elbow Ramy El Nakeeb, MD. Orthopaedic Department Damanhour Medical institute
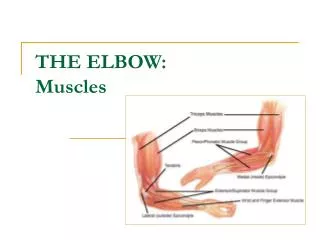
Lateral Epicondylitis (tennis elbow) • Definition: • “Tendinopathy of the common extensor origin of the elbow” • Pathology • 30 – 50 years old • Repetitive micro-trauma • Chronic tear in the origin of the extensor carpiradialisbrevis
Tendinosis • Mucoid degeneration • Loss of collagen tight bundled structure • Fibrosis • Neo-vascularisation (Khan et al. 1999)
Mechanism of Injury: Overuse syndrome caused by repeated forceful wrist movements • Tennis players • Prolonged and rapid activities
Symptoms • Increased pain around lateral epicondyle • Weakness • Difficulty doing normal daily tasks
Clinical Signs • Pain on palpation in the area just distal to the lateral epicondyl (Common extensor tendon) • Pain on Resisted elbow extension • Lidocaine injection
Medial Epicondylitis (golfer’s elbow) The medial condyle of the humerus gives origin to the flexor-pronator origin, including the pronatorteres, the flexor carpiradialis, the humeral head of the flexor ulnaris, the palmarislongus, and the ulnar head of the flexor digitorumsuperficialis. The pronatorteres and the flexor carpiradialis share a conjoined tendon that is regarded as the primary site of origin of this condition.
Pathology • 30 - 50 years old • With repetitive stress loading of this conjoined tendon(Repetitive micro trauma ) , degenerative changes occur in the tendon leading to pain.
Mechanisms of injury • Racquetball or tennis • Swimming backstroke • Hitting a golf ball
Symptoms • Increased pain over medial epicondyle • In some cases, patients complain of associated ulnar neuropathy.S
Signs • Tenderness over the medial humeral condyle can be elicited on physical examination. • Pain with resistive forearm pronation is also variably present. • Elbow range of motion is usually preserved but grip strength may wane. • Lidocaine
Treatment Treatment considerations for medial and lateral epicondylitis are similar and are considered together. The treatment of epicondylitis is controversial
Non-operative • Rest • NSAIDs • Physiotherapy • USS • Injection therapy Operative • Debridement of the diseased tendon
Nonoperative therapy is the main treatment option for medial and lateral epicondylitis. It has been suggested that greater than 85% to 90% of patients respond to nonoperative treatment • Activity modification is one of the mainstays of treatment, with avoidance of precipitating motions
NSAIDs • Insufficient evidence to recommend or discourage the use of oral NSAIDs • No conclusion regarding oral versus topical
Physiotherapy • Principles: • Eccentric loading • Close to limit of tendon without exceeding it • Avoid exacerbating activities
Physiotherapy Bisset et al BMJ 2006 • 52 week FU • No better outcome than “wait and see” • BUT took less adjunctive medications Tyler et al JSES 2010 • Eccentric exercises beneficial • 7 weeks only FU
Cortisone Injections • Common treatment • Short-term improvement (6-8 weeks) • Beneficial with degenerative pathology • local side-effects
Injection of blood products • Attempt to address pathology • Growth Factors e.g. TGF-ß + FGF • Autologous blood • Platelet Rich Plasma (PRP) • Bone Marrow Aspirate
When patients present for evaluation and treatment of epicondylitis, they often expect some active intervention. Based on the available evidence, most cases resolve with patience and minimal intervention within 18 months, and probably the best recommendation for treatment is oral analgesics for symptom relief, modifying one's behavior (at work and at play), and waiting things out for 18 months. In some ways, it is unrealistic, however, to expect most patients to accept and wait till the pain resolves on its own, and that leaving things be and allowing significant time for healing is sufficient treatment.
Heal with Steel? • Reserved for refractory cases • Debridement of abnormal tendon of ERCB
Conclusion In lateral and medial epicondylitis, most patients respond to nonoperative therapy (activity modifications with or without adjunctive measures) after up to 18 months. ▪ Little evidence exists regarding the efficacy of adjunctive nonoperative therapies over placebo; however, they are widely used and may give the patient satisfaction and some subjective benefit in pursuing an “active” treatment.
▪ Operative treatment may be considered after more than 6 months of recalcitrant symptoms; in medial epicondylitis, presence of acute avulsion of the flexor pronator origin, worsening ulnar neuritis, or MCL insufficiency are also indications for surgery. ▪ In open lateral epicondylitis surgery and medial epicondylitis surgery, the abnormal tissue is identified as a gray, friable, edematous tendon and is excised. ▪ The origins are repaired as indicated, and resisted wrist motion is avoided postoperatively.
An inability to oppose the thumb to the little finger can result from damage to the ________ nerve. • Axillary • Musculocutaneous • Radial • Ulnar • Median
Hyperextension of the proximal phalanges of the little and ring fingers can result from damage to the ________ nerve. • Ulnar • Axillary • Radial • Median • Musculocutaneous
Wrist drop can result from damage to the ________ nerve. • Median • Ulnar • Radial • Anterior interosseous • Axillary
Tendon Transfers • Definition • The Detachment Of A Functioning Muscle-Tendon Unit From Its Insertion And Reattachment To Another Tendon Or Bone To Replace The Function Of A Paralyzed Muscle Or Injured Tendon
Tendon TransfersRadial Nerve Palsy • PT ECRB • Wrist 45° Extension • Tendon Sutured With Maximal Tension • FCU EDC • Wrist and MP Joints In Neutral • Adjust EDC Tension Individually • +/- EDM • PL EPL • Wrist In Neutral • Maximal Tension On EPL And PL
Tendon TransfersRadial Nerve Palsy • FCR EDC • PT ECRB, When Required • Performed As Before • PL EPL • Performed As Before • If Absent • EPL Joined With EDC To FCR Transfer
Tendon TransfersMedian Nerve Palsy • Reconstructive Goals • Thumb Opposition • FPL Function • Index FDP Function • Sensation • Prime Determinant In Hand Function
Tendon TransfersMedian Nerve Palsy • Classification • High • Above Origin Of Anterior Interosseous Nerve • Pronator Teres And Quadratus, FCR, FDS (II – V), FDP(II & III) And FPL Paralyzed • Low • Thenar Intrinsic Muscles Paralyzed • Abductor Pollicis Brevis, Opponens Pollicis, And Superficial Head Of Flexor Pollicis Brevis
Tendon TransfersLow Median Nerve Palsy • Prevention Of Contractures • Good Therapy And Splinting • Position Of Thumb • Supinated And Adducted • Contracted First Web Space • Correct Contracture Before Opponensplasty • Release Fascia Over Adductor Pollicis And First Dorsal Interosseous
Tendon TransfersLow Median Nerve Palsy • Pulley Design • Straight Line Of Pull • Reduced Friction And Work • Tendon Migrates To Run In Straight Line
Tendon TransfersLow Median Nerve Palsy • Standard Opponensplasties • FDS Opponensplasty • Royle-Thompson Technique • Bunnell Technique • Extensor Indicis Proprius Opponensplasty • Huber Transfer • Abductor Digiti Minimi • Camitz Procedure • Palmaris Longus
Tendon TransfersHigh Median Nerve Palsy • Deficit • All Flexor Compartment Forearm Muscles • Apart From Ulnar-Innervated FCU And FDP • Aim Of Tendon Transfers • Flexion Of Index And Thumb • Opposition • Potential Motors • Brachioradialis FPL • ECRL Index FDP
Tendon TransfersHigh Median Nerve Palsy • Extrinsic Transfers • Restoration Of Index Function • ECRL Index FDP • Side-To-Side Suturing Of Profundus Tendons • Restores Range Of Motion • Strength Is Not Restored • Restoration Of Thumb Function • Brachioradialis FPL
Tendon TransfersUlnar Nerve Palsy • Classification • Low • Below Innervation To FCU And FDP (III & IV) • Affected Muscles • Seven Interossei, Ulnar Two Lumbricals, Hypothenar Muscles, And Adductor Pollicis • “Claw Deformity” • High • FCU And FDP (III & IV) Affected
Tendon TransfersUlnar Nerve Palsy • Clawing Of Fingers • Surgical Options • Capsulodesis • Prevent MCP Hyperextension • Described By Zancolli • Static Tenodesis (Parkes) • Prevents MCP Hyperextension • Provides IP Extension • Free Tendon Graft: Radial Lateral Band Dorsal Expansion