Fetal Membranes 2
390 likes | 1.86k Views
Fetal Membranes 2. Dr Rania Gabr. Objectives. By the end of this lecture, the student should be able to: Describe the structure, functions, anomalies of the placenta Describe the structure, functions, anomalies of the umbilical cord. PLACENTA. SHAPE: circular disc

Fetal Membranes 2
E N D
Presentation Transcript
Fetal Membranes 2 Dr Rania Gabr
Objectives By the end of this lecture, the student should be able to: • Describe the structure, functions, anomalies of the placenta • Describe the structure, functions, anomalies of the umbilical cord
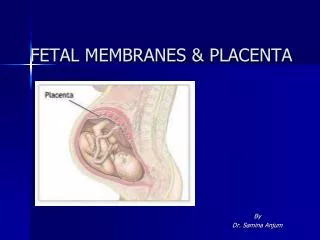
PLACENTA • SHAPE: circular disc • WEIGHT: about one-sixth that of fetus (500-600 gm) • DIAMETER: 15-20 cm • THICKNESS: 2-3 cm • SURFACES: 1. Fetal surface: smooth, transparent, covered by amnion with umbilical cord attached near its center & umbilical vessels radiating from it 2. Maternal surface: irregular, divided into convex areas (cotyledons)
PLACENTA • The maternal part of placenta is divided into cotyledons by projections from decidua basalis(placental septa) • Each cotyledon contains 2 or more stem villi with their branch villi • By the end of 4th month, decidua basalis is almost entirely replaced by cotyledons
PLACENTAL CIRCULATION • Poorly oxygenated blood leaves the fetus & passes through the 2 umbilical arteries to the placenta • Umbilical arteries divide into several chorionic arteries that enter chorionic villi • An arterio-capillary-venous network is formed in chorionic villi • Exchange of materials between fetal & maternal blood (in intervillous spaces) occurs across placental membrane (barrier) • Oxygenated blood returns to fetus by umbilical vein
Functions of the Placenta • Exchange of metabolic & gaseous productsbetween maternal & fetal bloodstreams • Respiratory function: Exchange of gases – • Nutritive function: Exchange of nutrients & electrolytes – • Transmission of maternal antibodies – • Excretory function: Co2 and other stuff • Barrier function: prevents passage of some bacteria and some drugs from maternal to fetal blood.
Endocrine function: Production of hormones • Protein hormones: • Human chorionic gonadotropin(early pregnancy tests) • Human placental lactogen • Human chorionic thyrotropin • Human chorionic corticotropin • Relaxin • Steroid hormones: • Progesterone • Estrogen
ANOMALIES OF PLACENTA • ANOMALIES IN SIZE & SHAPE: • Normally chorionic villi persist only at site of decidualbasalis: • Placenta membranacea: a large thin membranous placenta due to persistence of functioning villi on the entire surface of chorionic sac • Accessory placenta: a patch of chorionic villi persisted a short distance from main placenta
ANOMALIES OF PLACENTA • ANOMALIES IN POSITION: • Placenta previa: when blastocyst implants close to or overlying internal os of uterus late pregnancy bleeding • ANOMALIES IN EXTENSION: • Placenta accreta: chorionic villi extend to the myometrium • Placenta percreta: chorionic villi penetrate the whole thickness of myometrium & extend to perimetrium
ANOMALIES OF PLACENTA • ANOMALIES IN ATTACHMENT OF UMBILICAL CORD: • Battledore placenta: the cord is attached to the margin of placenta • Velamentous insertion of cord: the cord is attached to the membranes surrounding placenta, umbilical vessels are liable to be ruptured
Battledore placenta Velamentous insertion of cord
Umbilical Cord • Cord like structure • Connects fetus to the placenta • Attached to the ventral surface of the fetal body and to the smooth chorionic plate of the placenta
Umbilical Cord: Formation • Develops from the connecting stalk • The connecting stalk initially attached to the caudal end of the embryonic disc, after folding, becomes attached to the ventral surface of the curved embryonic disc, at the umbilical region • Theumbilical region wider initially, becomes narrower as the folding progresses • The underlying structures are compressed together and form a cord like structure, the umbilical cord
Umbilical Cord: Formation cont’d • Initial contents: • Connecting stalk • Umbilical vessels • Allantois • Yolk sac • Extraembryoniccelome • Intestinal loop (during 6-10 weeks)
Umbilical Cord: At Term At term, the typical umbilical cord: • Is 55-60 cm in length,with adiameter of 2-2.5 cm • Hasknottyappearance • Usually contains two arteriesandone vein • Issurrounded by a jelly like substance called the Wharton's jelly • Is enclosed in amnion amnion
Umbilical Cord: Placental Attachment May attach to the placenta near its margin- Marginal attachment Typically attaches to the placenta near its center- Eccentric attachment placenta May attach to the membranes around the placenta- Membranous (Velamentous ) attachment
Umbilical Cord cont’d • After delivery of the placenta the umbilical cord is usually clamped and severed • The site of its attachment leaves a scar, the navel (belly button), on the anterior wall of the abdomen
Abnormalities Related to Umbilical Cord • Omphalocele: Failure of returning of intestinal loops back into the abdominal cavity • Long cord may prolapse or coil around the fetus thus cause difficulty in labour • Short cord may result in premature pull and separation of placenta causing severe bleeding during birth • True knots True knot Prolapsed cord