Download
1 / 75
770 likes | 981 Views
Brain Tumors: Epidemiology and Principles of Diagnosis and Management. Andrew J. Tsung M.D. Patrick W. Elwood Endowed Assistant Professor Department of Neurosurgery Director, Brain Tumor Center and Neurosurgical Research Illinois Neurological Institute

E N D
Brain Tumors: Epidemiology and Principles of Diagnosis and Management Andrew J. Tsung M.D. Patrick W. Elwood Endowed Assistant Professor Department of Neurosurgery Director, Brain Tumor Center and Neurosurgical Research Illinois Neurological Institute University of Illinois College of Medicine at Peoria
Continuing Education Provider OSF Saint Francis Medical Center Continuing Education Provider Program (CEPP) is an approved provider of continuing nursing education by the Illinois Nurses Association, an accredited approver by the American Nurses Credentialing Center’s Commission on Accreditation.
Conflict of Interest There is no conflict of interest or bias on the part of the presenter.
Objectives • Describe the epidemiology of brain tumors • Categorization of tumors • Brief description of only the most commonprimary brain tumors • Management of metastatic brain cancer • Familiarity with methods of current diagnosis • Imaging • Physical Examination • Options in surgical management • Surgery • Craniotomy • Stereotactic biopsy • Radiation • Radiosurgery (single fraction i.e. gamma knife) • Whole brain radiotherapy (multiple fractions/non-conformal) • Fractionated radiotherapy (multiple fractions/conformal) • Identify complications- surgical and non-surgical • Summary
Primary Concepts • Primary Brain Tumors • Meningiomas can be treated effectively with gamma knife or surgery • Glioblastoma is uniformly fatal, but we are making progress, necessitating full evaluation. Aggressive surgery and chemoradiation therapy provides survival benefit. A nihilistic approach is never appropriate regardless of age • WBRT solely is not the “easy” solution to metastatic brain cancer due to prolonged survival
Epidemiology-Overall Numbers • Primary brain tumors • 43,000 annually and 13,000 people die • 1.5 million diagnosed with diabetes in the U.S. alone • Overall annual incidence in the U.S. is 15/100,000 • Overall annual incidence for primary malignant is 7/100,000 • Brain tumors are increasing dramatically over the past 3 decades (300%) • Improved diagnostic capabilities (CT/MRI) • Changing attitudes towards diagnosis in the elderly • There may be inherent causal factors, especially in children
Epidemiology-Age and Gender • Gender variation among tumor types • Most significant is glioma vs meningioma
Epidemiology-Age and Gender • Overall median age of onset of primary brain tumors is 57 • GBM and meningioma 64/63, respectively • Most common types of gliomas (GBM and astrocytoma) contribute to the peak observed at ages 75-84 • Meningioma increases continuously with age
Epidemiology-Survival and Prognostic Factors • Survival has not significantly changed for the last 30 years for patients with glioblastoma multiforme (GBM) –Disagree!! • Some notable improvements have been reported for medulloblastoma • Overall, rates vary significantly among different types of tumors • Histologic type and age are generally the strongest prognostic factors • Reasons for variation even within histologic subcategory: • Tumor/molecular markers • 1p/19q • EGFR amplification • MGMT methylation
Epidemiology-Risk Factors • Head trauma- meningioma, no link with other tumors • Subject to recall bias • Exposures to drugs/medications • Very few studies • Diet/Vitamins/Alcohol/Tobaco/Residential Chemicals • N-nitroso compounds (cured meats) • Probable but not definite link in a meta-analysis of nine studies suggest a 48% increase in risk • Smoke all you want (as long as they are filtered) • Alcohol may give you a subdural when you fall off the barstool, but not a GBM
Epidemiology-Risk Factors • Industry and Occupational Chemicals • No definite link to a certain chemical • Industries in the Texas petrochemical plants suggested higher malignant brain tumors • Manufacturing of pesticides or fertilizers • Rubber/tire industries • Laboratory scientists • Ionizing Radiation • Strong link • Tinea capitis (1.5 Gy) results in relative risk of 18,10, and 3 for nerve sheath tumors, meningioma, and gliomas • Prophylaxis for ALL • Atomic bomb survivors and meningioma • Parental exposure to radiation prior conception not a risk factor • Prenatal exposure unclear (mostly involve dental xrays and meningioma with increased risk of 1.2-3.0 • Cellular phones and EMF • No definite link • Most do not show any link • One long-term study (10 years) of cell phone use showed a 2x increased risk for acoustic neuroma (vestibular schwannoma), when restricted to the ear of use, risk increased 4x • RF frequencies have changed though, analog is 800-900 MHz while digital operates in the range of 1600-2000 MHz • EMF • 52 studies reviewed, inclusion of 29 studies in a meta-analysis that showed a significant increased risk of 10-20% • San Francisco population based study reviewed 492 patients with glioma who were not more likely than 463 controls to have lived near high wires during 7 years prior to diagnosis • Problem exists that the pertinent exposure period is unknown (as the mechanism of tumorigenesis is unknown)
Epidemiology • Genetic predispostion-What does this mean? A single gene or multifactorial increased susceptibility? • Susceptibility implies genetic alterations than influence oxidative metabolism, carcinogen detoxification, DNA stability and repair, immune response, and other aspects of metabolism and cellular function • Evidence is clear- genetics play a role, but only account for 5-10% of brain tumors • Hereditary syndromes • Li-Fraumeni syndrome • First degree relative with cancer 58 vs 42% • Previous history of cancer 17 vs 8%
Categorization • World Health Organization of CNS Tumors • 9 Major Categories • Tumors of neuroepithelial tissue represent a significant portion of primary brain tumors • “Glioma” often used to refer to glial tumors of any glial lineage but in its usual sense, we mean only astrocytic tumors
Common Tumor Types and Characteristics • Low grade astrocytoma • Histologic Subtypes • Fibrillary • Protoplasmic • Gemistocytic • Diagnosis • Majority present with seizures >50% • Treatment - Controversial • Observation, no difference in survival if surgery is deferred until growth, transformation, intractable seizures • Resection, gross total or biopsy ± radiation • Favored at Neurosurgical Oncology centers • Radiation- may improve time to progression without survival benefit, may be delayed until progression is seen • Prognosis • Median survival 8-12 years • Prognostic factors Age, enhancement, KPS
Patient Example • 20 yo healthy male presenting with first time GTC seizure, no focal deficit • Biopsy via awake craniotomy, positive speech arrest at periphery and surgery terminated • Grade 2 Astrocytoma • No further adjuvant treatment
Patient Example August 2007 December 2010
Patient Example Patient discharged home POD 3 No deficit Pathology Grade 3 Anaplastic Astrocytoma Must now undergo chemo and radiation
Common Tumors • Anaplastic Astrocytoma and GBM aka “Malignant Glioma”
Common Tumors • AA/GBM • Median age 60 yo • Seizures in 20% • AA 30% nonenhancing/GBM 4% nonenhancing • Treatment • Surgical resection followed by conformal XRT and concomitant temozolomide (Temodar) • “Stupp” Protocol Standard of care since 2006
Common Tumors • AA/GBM
Questions about AA/GBM • How much does surgery help? • Does “good” surgery help more? • How much does age affect the outcomes? • Have we made any progress?
Pushing the limits • 73 yo male professor presents with headache only • Mayo Clinic Neurosurgery refused surgical intervention due to high risk • Was biopsied only at MC, however too small of specimen taken to enroll in any clinical trials
Pushing the limits • Resected at the INI and discharged without complication 2 days after surgery • 95-98% resection • Undergoing chemoradiation therapy with KPS 80 • Did we do the right thing?
Comparison to other cancers Median PFS
Comparison to other cancers Median OS
Common Tumors • Meningioma • Arise from arachnoid cap cells • Increases with age • Incidence 0.3/100,000 in childhood to 8.4/100,000 in elderly population • Female 2:1 • Locations Parasagital>convexity>sphenoid wing • May have increased risk with HRT • Symptoms • Non-focal from increase in ICP • Seizures (up to 40%) • Localized CN deficit or compression upon eloquent areas depending on the location of the tumors • Histologic grades • Grade I/II/III • Indicate the malignancy and thus the propensity to recur after resection
Common Tumors • Meningioma • Surgery is the mainstay of treatment for symptomatic patients • Not all need to be treated • Availability and frequency of scanning results in high numbers of incidental meningiomas (2.3% in autopsy series) • Commonly thought that they do not grow throughout life and have very low rates of growth (between 0.03 and 2.62 cc/year) • Elderly show lower growth rates than those in younger people • Asymptomatic tumors are occasionally removed depending on location • If further growth would result in great difficulty in surgical removal • Have displayed high growth rates on follow-up imaging • Observation, radiosurgery (gamma knife) or radiation therapy for subtotal resection (approximately 1 in 3 are not fully resectable, with even higher rates when involving the skull base) • Modern results with resection and subsequent radiotherapy show control rates of 91-100% at 5 and 10 years with acceptably low complication rates (<6%)
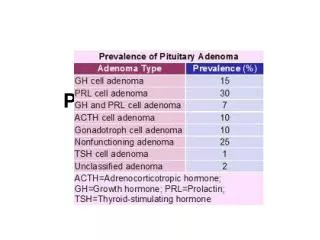
Common Tumors • Pituitary Adenoma • Pituitary is the master gland regulating most of the body’s hormonal balance secreting prolactin (Prl), growth hormone (GH), thyroid stimulating hormone (TSH) gonadotropic hormones (FSH/LH), and adrenocorticotropic hormone (ACTH), oxytocin and ADH • 10-15% of intracranial neoplasms • 3rd most common after glioma and meningiomas • Many are asymptomatic, review of autopsy and radiographic studies reveal 16% with pituitary lesions • Increases with age • Classically divided into two groups, functional or non-functional • Prolactin>Null cell>GH>ACTH • Presentation • Endocrinologic disturbance, usually prolactin with amenorrhea/galactorrhea/sexual dysfunction or GH and acromegalic features (increasing hand/foot size, coarse facial features, frontal bossing, prognathism, macroglossia) • Mass effect-Primarily visual loss • Pituitary apoplexy – Headache, visual loss, CN palsy, hypotension • Hypopituitarism 75% hypogonadal, 36% hypoadrenal, 18% hypothyroid
Common Tumors • Pituitary Adenoma • Management • Prolactinoma-Dopamine agonists (Bromocriptine, Dostinex), surgery for failure • GH, ACTH, Non-functioning-Surgery • Surgery performed via transphenoidal approach • Radiotherapy for residual tumor in certain circumstances (long term chance of hypopituitarism approaches 40%), appropriate approach may be observation until recurrence
Common Tumors • Pituitary Adenoma
Brain metastases • According to 2008 American Cancer Society Registry, 1.4 million Americans diagnosed with cancer every year • Average survival 3-6 mo with radiation alone • Extended survival to approx 12 mo with surgery and radiation treatment • 40% or >500,000 will develop brain metastases • 1/3 of these patients are surgical resection candidates
Brain metastases • General conditions: • <3 cm asymptomatic with known primary cancer with imaging characteristics consistent with mets then Gamma knife, conformal radation (IMRT)or WBRT plus gamma knife boost can be used
Brain metastases • Surgery should be considered first line for: • Any lesion greater than 3 cm • Any symptomatic lesion regardless of size • Any lesion near eloquent regions (motor cortex, visual regions, speech, or optic nerves) • Questionable primary cancer diagnosis • Very remote history of cancer • Pathology not known to metastasize to brain • Failure of radiation therapy • Persisting corticosteroid requirement • Palliative for mass effect and symptom relief
Evidence? • Level 1Evidence • Surgical resection plus WBRT versus surgical alone • Good performance status (functionally independent, less than 50% of time in bed), KPS >70 • Limited extra-cranial disease • Insufficient evidence to make a recommendation for patients with poor performance scores, advanced systemic dz, or multiple brain mets
Not everyone fits the guidelines – patient example • 68 yo female h/o breast Ca. Systemic disease controlled. Poor performance status due to hemiparesis • 2.9 cm mass in eloquent region – thalamus, superior brainstem • Very difficult surgical access with high potential for complication if not performed with precision
Patient Example • Post operative weakness requiring rehab for 2 weeks • Improved and discharged home. At 1 month, fully independent with minor left hand dexterity complaints, 4+/5 strength • Stereotactic conformal fractionated (5 fx) treatment to resection cavity only • Alive with KPS 90 8 months post-op. No systemic disease progression • Would fractionated treatment alone have provided same benefit? • If she had WBRT, would she have started developing the late cognitive deficits (>12% at 1 year) given her likely long-term survival? • Were we “lucky” at surgery?
Summary • Don’t believe every low survival statistic, data is based on only Level 1 evidence from 1 single RCT completed in 1998, over ten years ago and not powered to detect OS as an endpoint • WBRT is toxic over long term and should be avoided if other methods can be used, thus concurrent evaluation by radiation oncology AND neurosurgical oncology warranted • Survival is dictated by systemic disease status, patients only die from CNS progression in 1/10 cases. Thus, certain pathology (breast) warrant a more aggressive surgical and focal radiation strategy • Given low complication rate from craniotomy, palliation of symptoms and prolonged maintenance of QOL via surgical resection for large masses must always be considered, even those with advanced systemic disease
Radiosurgery/Radiotherapy • Gamma Knife radiosurgery • Whole brain radiotherapy • Fractionated conformal radiotherapy
Diagnosis-Signs and Symptoms • Variability depending on tumor type, and thus typical location, growth pattern, seizure propensity, etc. • Most common presentation is progressive neurologic deficit, 68% and motor weakness, 45%, headache in 54%, seizures in 26% • Supratentorial • Increased ICP • Mass effect of tumor and/or edema • Blockage of CSF drainage (hydrocephalus) • Progressive focal deficit including weakness and aphasias • Destruction of brain tissue • Compression of brain tissue by mass/edema/or hemorrhage • Compression of cranial nerves • Headaches • With or without increased ICP • Classic: Worse in the morning • Worse with cough, straining, bending forward • Associate with nausea/emesis • Only 8% present with “Classic” brain tumor headache • Variable presentations • Etiology • Increased ICP • Invasion of dura, blood vessels, periosteum • Secondary to difficulty with vision from CN dysfunction (3,4,6) • Hypertension with or without presence of Cushing’s Triad • Psychogenic