Download
1 / 30
310 likes | 343 Views
Explore drug therapy options for osteoporosis including bisphosphonates, estrogen, and calcitonin. Learn about research findings on Alendronate, Risedronate, and Ibandronate, and clinical advice for bisphosphonate use. Understand hormone therapy history, effectiveness, and associated risks.

E N D
OsteoporosisPart 3 of 3: Treatment Ellen Davis-Hall, PhD, PA-C Professor Clare J. Kennedy, MPAS, PA-C Assistant Professor, PA Program SAHP , COM UNMC Omaha, NE. office: 402-559-4738 email: clarekennedy@unmc.edu
PROCESS Series of modules and questions Step #1: Power point module with voice overlay Step #2: Case-based question and answer Step # 3: Proceed to additional modules or take a break
Objectives • Part 1: Identify risk factors for osteoporosis with an emphasis on modifiable risk factors • Part 2: Describe the most current methods of, and standards for, diagnosis and monitoring of treatment • Part 3: Describe the available treatment modalities for osteoporosis and their effectiveness
Drug Therapy Options for Osteoporosis • Antiresorptive agents • Anabolic agents
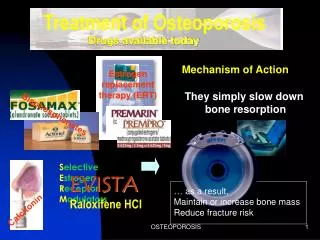
Antiresorptive Agents • Bisphosphonates • Estrogen • Selective estrogen receptor modulators (SERMs) • Calcitonin
Bisphosphonates-Non-hormone Compounds • Alendronate (Fosamax) • Risendronate (Actonel) • Ibandronate (Boniva)
Alendronate (Fosamax) Research • Spinal BMD increases of 6-8%, and hip increases of 3-6% over three years. (Black, et al 1996) • 50% reduction in fracture risk for spine, hip and wrist (Cranney et al 2002a) • Benefits seen as early as 1 year for spinal fractures and 18 months for hip fractures (Black et all 2000) • 95% of women who take alendronate maintain or increase bone mass (Black et al, 2000) • Benefits seem to continue even 2 years after med is stopped (Tonino et al, 2000) • Also approved for treatment of male osteoporosis and prevention of steroid induced osteoporosis
Risedronate (Actonel) Research • Increases BMD and reduce fracture risk significantly • Increases spine BMD by approximately 5% and hip BMD by 2-3% (Harris et al, 1999) • 41% reduction in spine fractures; 39% reduction in non-spine fractures; and 30% reduction in hip fractures (Harris et a, 1999; McClung et al, 2001) • Reductions in spine fractures can be seen after one year of therapy(Harris et al, 1999) • Approved for treatment of osteoporosis, osteopenic post-menopausal women, and prevention and treatment of steroid induced osteoporosis
Ibandronate (Boniva) Research • Chesnut (2004) • Daily oral dose of 2.5 mg compared with “intermittent administration” • “Intermittent administration” consisted of 20 mg every other day for 12 doses given every three months • No difference was noted from placebo in regard to GI side effects • Vertebral fracture risk was reduced by 62% with daily dosing • Vertebral fracture risk was reduced by 50% with intermittent dosing • May hold promise as an effective and convenient alternative to current bisphosphonate therapies
Clinical Advice for Bisphosphonate Use • Morning dosing, empty stomach, full glass of water • No food or other liquids other than water for 30 minutes • Should not lie down during this period • Proceed cautiously when prescribing to patients with: • known history of esophageal narrowing or ulcers of the esophagus • long term problems with stomach ulcer • heartburn that requires medication
Hormone Therapy • In 1942 conjugated equine estrogen (CEE) was approved for the relief of menopausal symptoms • In 1972 use extended to postmenopausal osteoporosis • Early 1970s observation that estrogen was associated with an increased risk of endometrial cancer • PEPI (Postmenopausal Estrogen/Progestin Interventions, 1996) and HOPE (Women’s Health, Osteoporosis, Progestin, Estrogen, 2002) studies demonstrated that postmenopausal hormone therapy had a favorable effect on BMD at all sites • spine (3.5 to 7%) • hip (2 to 4%) • forearm (3 to 4.5%) • Increases apparent after 1 year use • No differences in estrogen formulations
Estrogen and Fracture Risk • Research mostly observational studies • Meta-analyses suggest • Estrogen reduces the risk of non-spine fractures by 27% • Estrogen reduces the risk of spinal fractures by 33% (Torgerson and Bell-Syer, 2001)
Women’s Health Initiative (WHI) • 1990s: Trials designed to answer questions about hormones • Two separate trials: • women with an intact uterus • women post-hysterectomy • Treatment: • Intact uterus group treated with CEE and medroxyprogesterone (MPA) • Post-hysterectomy group treated with CEE alone • Hip and spine fractures were reduced by one-third in both groups • Other results: • increased risk of stroke, cognitive impairment, and deep vein thrombosis in the women taking HT • No clear cardiovascular benefit was found • Breast cancer risk was increased (Cauley, et al, 2003)
Decision Factors in Hormone Use • Weigh known benefits against known risks • Hormone therapy still appropriate for women with osteoporosis who cannot tolerate other medications • Perimenopausal women currently advised to take lowest dose possible for as short a time as necessary to achieve treatment goals • Even low doses of hormones are effective at preserving bone density • No long term benefit exists once discontinued • Goal of hormone therapy: Capture positive effects without incurring deleterious effects
Selective Estrogen Receptor Modulators (SERMs) • Called “designer estrogens” • Interact with estrogen receptors located throughout the body. • Provide benefits of estrogen without some of the negative effects (Ettinger et al, 1999)
Raloxifen (Evista) Research • Spine BMD increased 2-3% and hip BMD by 2.5% after three years.(Ettinger et al, 1999) • Spine fractures reduced by 50%, but no effect was noted on hip or other non-spine fractures (Ettinger et al, 1999, Cranney et al 2002) • Spine fracture reduction achieved at one year (Maricic et al, 2002) • No long term fracture benefit once discontinued • Other potential benefits • decrease in total cholesterol and LDL • possible decreased incidence of breast Cancer
Raloxifen Use • Approved for prevention and treatment of postmenopausal osteoporosis at a dose of 60 mg/day • Side effects: • a possible return or exacerbation of hot flashes • blood clots in the legs, and/or lungs. • Drug should be discontinued if the patient is immobilized for long periods of time
Calcitonin (Miacalcin) • Inhibits bone resorption by directly inhibiting osteoclasts • In 1970s and 1980s calcitonin was administered by subcutaneous injection • Calcitonin now available as a nasal spray • Prevent Recurrence of Osteoporotic Fractures (PROOF) trial found a decline of spinal fracture of 33% • No significant differences for non-spine fractures • Calcitonin has a unique pain-relief benefit for acute spinal fractures • Dose: 200 IU/day ( 1 spray, alternate nostrils) • Side effects: nasal stuffiness, nausea, dry mouth (Chesnut et al, 2000)
Antiresorptive Summary • Bisphosphonates (caution in those with esophageal problems) • Hormones (weigh benefits against risks) • SERM (may increase hot flashes) • Calcitonin (decreases spinal fractures, and provides some pain relief of these fractures)
Recent Concerns with Bisphosphonates • Severe bone, joint and/or muscle pain have been reported.(Wysowski and Chang, 2005) • Osteonecrosis of the jaw recently reported (Ruggiero, et al 2004; Carter and Goss, 2003; Starck and Epker, 1995) • Ocular inflammation has been reported (Fraunfelder and Fraunfelder, 2003) • Long term bone strength has been called into question (Odvina et al, 2005). • It has been suggested that bisphosphonate therapy be discontinued after 5 years (Medical Letter, 2005)
Anabolic Agents • Parathyroid hormone • Fluoride • Growth hormone • Statins • Insulin-like growth factor (IGF-1)
Anabolic Agents:Parathyroid Hormone (PTH) • Teriparatide (Forteo) Eli Lilly and Company recombinant human PTH (1-34) • Stimulates new bone formation • Increases bone mass • Increases trabecular connectivity • Increases mechanical strength • 20 micrograms given once daily subcutaneously for up to 2 years-with sustained effect thereafter • Increases vertebral, femoral, and total-body mineral density and is well tolerated (Neer, et al, 2001)
Anabolic Agents-Fluoride • One of the first treatments for osteoporosis • Increases spine bone density but does not necessarily reduce fracture risk • Builds bone, but bone is more “brittle” • May even cause increased appendicular fractures • Research is conflicting and controversial • May prove useful in combination with a bisphosphonate, but further research is needed
Summary of Part 3: Treatment • Antiresorptive therapies are our primary treatment for osteoporosis, most notably the bisphosphonates • Recent data is calling into question the quality of the bone resultant from bisphosphonate therapy • Consideration might be given to discontinue this drug after 5 years of therapy • Research is ongoing for newer pharmacological agents
The End of Module Three on Osteoporosis References • Black et al, Randomized trial of effect of alendronate on risk of fracture in women with existing vertebral fractures. Fracture Intervention Trial Research Group. Lancet 1996, Dec 7;348(9041):1535-41 • Black et al, Fracture risk reduction with alendronate in women with osteoporosis: the Fracture Intervention Trial Research Group. J Clin Endocrinol Metab 2000 Nov;85(11):4118-24 • Brett, A. Is long term bisphsphonate therapy safe? Medical Letter, 2005 May 1;25(9) • Carter et al, Bisphosphonates and avascular necrosis of the jaws. Aust Dent J 2003;48:268 • Cauley et al, Women’s Health Initiative Investigators. Effects of estrogen plus progestin on risk of fracture and bone mineral density: The Women’s Health Initiative Randomized Trial. JAMA 2003 Oct 1:290(13):1729-38 • Chesnut et al, A randomized trial of nasal spray salmon calcitonin in postmenopausal women with established osteoporosis: The Preventive Recurrence of Osteoporotic Fractures study. PROOF Study Group. Am J Med 2000, Sep;109(4):267-76
References • Chesnut et al, Effects of oral ibandronate administered daily or intermittently on fracture risk in postmenopausal osteoporosis. J of Bone and Min Res 2004, March; 19(8):1241-49 • Cranney et al, Osteoporosis methodology group and the osteoporosis research advisory group. Meta-analyses of therapies for postmenopausal osteoporosis. II Meta-analysis of alendronate for the treatment of postmenopausal women. Endocr Rev 2002, Aug;23(4):508-16 • Ettinger et al, Reduction of vertebral fracture risk in postmenopausal women with osteoporosis treated with raloxifene: Results from a 3-year randomized clinical trial. Multiple outcomes of raloxifene evaluation (MORE) investigators. JAMA 1999 Aug 18;282(7):637-45 • Fraunfelder & Fraunfelder, Bisphosphonates and ocular inflammation. N Engl J Med 2003; 348:1187 • Harris et al, Effects of risedronate treatment on vertebral and nonvertebral fractures in women with postmenopausal osteoporosis: A randomized controlled trial. Vertebral Efficacy with Risedronate Therapy (VERT) Study Group, JAMA 1999 Oct 13;282(14):1344-52
References • Lindsay et al. Effect of lower doses of conjugated equine estrogens with and without medroxyprogesterone acetate on bone in early postmenopausal women. JAMA 2002 May 22-29;287(20);2668-76 • Maricic et al, Early effects of raloxifene on clinical vertebral fractures at 12 months in postmenopausal women with osteoporosis. Arch Intern Med 2002 May 27;162(10):1140-3 • McClung et al, Effect of risedronate on the risk of hip fracture in elderly women. Hip Intervention Program Study Group. N Engl J Med 2001 Feb 1;344(5):333-40 • Neer, et al, Effect of parathyroid hormone (1-34) on fractures and bone mineral density in postmenopausal woman with osteoporosis. NEJM 2001, 344:1434-41 • Odvina et al, Severely suppressed bone turnover: A potential complication of alendronate therapy. J Clin Endocrinol Metab 2004 Dec 14 • Ruggiero, et al Osteonecrosis of the jaws associated with the use of bisphosphonates: a review of 63 cases. J Oral Maxillofac Surg 2004;62:527
References • Starck & Epker, Failure of osseointegrated dental implants after diphosphonate therapy for osteoporosis: A case report. Int J Oral Maxillofac Implants1995;10:74 • Tonino et al Skeletal benefits of alendronate: 7 year treatment of postmenopausal osteoporotic women. Phase III osteoporosis Treatment Study Group. J Clin Endocrinol Metab 2000 Sep;85(9):3109-15 • Torgerson et al, Hormone replacement therapy and prevention of nonvertebral fractures: A meta-analysis of randomized trials. JAMA 2001 Jun 13;285(22):2891-7 • Torgerson et al, Hormone replacement therapy and prevention of vertebral fractures: A meta-analysis of randomized trials. BMC Musculoskelet Disord 2001;2(1):7-10 • Writing Group for the PEPI. Effects of hormone therapy on bone mineral density: Results from the Postmenopausal estrogen/Progestin Interventions (PEPI) Trial. JAMA 1996 Nov 6;276(17):1389-96 • Wysowski & Chang, Alendronate and risedronate: Reports of severe bone, joint and muscle pain. Arch Intern Med 2005; 165:527
Post-test A 67 year old woman presents to your office with a DEXA score of -2.9. She has been told by her family doctor that she "should take a medication for her bones." She is currently being treated for mild hypertension with HCTZ and has a history of GERD under treatment with omeprazole. Family history is positive for breast cancer in her mother. The best drug treatment for this patient's osteoporosis is: • Alendronate • CEE/MPA • Raloxifene • Calcitonin