Download
1 / 34
340 likes | 539 Views
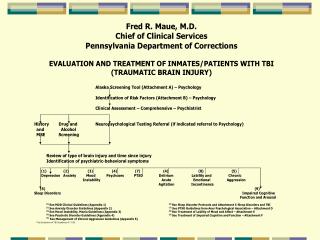
TBI - Neuroanatomy of TBA. Primary Effects: Diffuse Axonal Injury Contusions Secondary Effects: Hematomas Cerebral Edema Hydrocephatus Infections Neurotoxicity ↑ ICP Hypoxic or anoxic event. Prediction of Outcome after TBI. Injury severity Duration of Post-Traumatic Amnesia

E N D
TBI - Neuroanatomy of TBA • Primary Effects: • Diffuse Axonal Injury • Contusions • Secondary Effects: • Hematomas • Cerebral Edema • Hydrocephatus • Infections • Neurotoxicity • ↑ ICP • Hypoxic or anoxic event
Prediction of Outcomeafter TBI • Injury severity • Duration of Post-Traumatic Amnesia • Type of damage (contusion vs. DAI) • Premorbid intelligence • Alcohol intoxication at time of injury • Premorbid OBS or history of substance abuse • Premorbid psychiatric/behavioral history
TBI - Risk Factors for TBI • Men 2:1 • 15-24 Years Old • Alcohol • Trauma
TBI - Personality Changes – Common • Worsening of premorbid behavioral traits • Childishness • Disinhibition • Social inappropriateness • Restlessness • Emotional lability • Decreased social contact • Less spontaneity/poverty of interest • Decreased social interaction
TBI – Executive Function Changes – Decreased Mental Flexibility • Decreased capacity to: • Concentrate • Use language • Abstract calculate • Reason remember • Plan • Access information
Post Concussion Syndrome and TBI • Criteria: • Any period of LOC • Any loss of memory • Any alteration in mental status • Mild focal neurological deficits
Post Concussion andTBI Syndrome • Somatic: HA, dizziness, fatigue, insomnia • Cognitive: memory deficits, impaired concentration • Perceptual: tinnitus, noise sensitivity, light sensitivity • Emotional: depression, anxiety, irritability • Other: decreased reasoning, information processing, verbal learning, attention
TBI - Assessment • Neuropsychological Testing: • Attention • Concentration • Memory • Verbal Capacity • Executive Functions: • Problem Solving • Reasoning Abilities • Abstract Thinking • Planning
Psychiatric Complicationsof TBI • Depression • Mania and mood instability • Delirium: • Restlessness • Agitation • Confusion • Disorientation • Delusions – hallucinations • Usual during coma emergence • Sleep Disturbance • Psychoses • Anxiety • Personality Changes • Emotional Instability • Chronic Aggression and Violence
Post Concussion andTBI Workup • Comprehensive assessment • Validate cognitive and emotional problems • Treat both cognitive and emotional difficulties • Treat underlying anxiety and psychological symptoms
General Principles of Treatment • Review all current meds – indications • Examine current or potential side effects • OBS patients: increased sensitivity to side effects • Start low – go slow • Allow sufficient time to work • Reassessness medication need
TBI - Treatment of Depression See Depression Guidelines for MDD and Bipolar Depression • Tricyclic anticholinergic effects may impair cognition
TBI - Treatment of Mood Instability – Mania,Hypomania, Mixed See Treatment Guidelines. • Lithium levels – keep level less than 1.0
TBI - Treatment of Psychoses See Clinical Guidelines for Treatment of Psychoses. • Increased sensitivity to EPS • Atypicals – less EPS potential, greater metabolic side effects, OHD, CVA • Risperdal – higher EPS
TBI -Treatment of Chronic Aggression –Episodic Dyscontrol See Management of Chronic Aggression Guidelines.
TBI - Treatment of Lability of Mood and Affect • Emotional incontinence • Antidepressants are best choice: • Fluoxetine (20-80 mg/d) – Prozac • Sertraline (25-150 mg/d) – Zoloft • Nortriptyline (50-150 mg/d) – Pamelor • Effexor (150-450 mg/day) – higher doses needed to get NE effect
TBI - Treatment of Acute Aggression • Antipsychotic meds: Haldol, Geodan • Problems: EPS, Akathisia, Retardation of neuronal recovery • Benzodiazepines: • Disinihibition, hostility, ataxia confusion, sedation, decreased memory • Treatment of choice: • Haldol plus Ativan – lowest dose needed
TBI -Treatment of Impaired Cognitive Function and Arousal • Psychostimulants: • Dexedrine • Ritalin • Indications for stimulants: • ADD or ADHD • Anergy/Apathy • Rage outbursts • Emotional incontinence • Emotional irritability • Frontal Lobe Syndrome – left sided
TBI – Treatment of Cognitive Dysfunction and Arousal • Psychostimulants: • May increase neuronal recovery • Side effects: paranoia, dysphoria, anorexia, irritability, agitation, insomnia • Wellbutrin – alternative to stimulants, no lower seizer threshold on SL formulation • Cylert – no proven help • Concerta – liver toxicity • Provigil (modafinil): • Awake, alert, but no cognitive improvement • Used for narcolepsy
TBI – Treatment of Cognitive Dysfunction and Arousal • Dopamine agonist: • Symmetrel (Amantadine hcl) – dose 100-400 mg/d • Improves: arousal, attention, initiation, processing speed, and agitation • Drug of choice for management of agitation post TBI • Side Effects: Hallucinations, GI upset, low blood pressure, lower seizure threshold • Action: NMDA antagonism, release Dopamine to stimulate interaction of neurons
Sleep Disorders and TBI • 50% of TBI patients with pain • 27-56% of all patients with TBI • Common symptom of co-existing depression • Acute phase of TBI – diffuse disruption of cerebral functioning, direct physical damage to brain, secondary neuropathological events • Decreased REM and slow wave sleep • Increase awakening at night • Shortening of total sleep time: • Decrease or disappearance of deep sleep • DIMS – common in recent injury
Treatment of Sleep Disorders in TBI Patients • Melatonin – 3.0 to 7.5 mg at bedtime • Ambien (5 to 20 mgs.) – shorter activity, preserves REM sleep, decreased daytime effects • Chloral Hydrate – rapid sleep induction, increases total sleep time, potential for tolerance, narrow therapeutic window • Trazadone (Desyrel) – useful in depressed-TBI patients with insomnia
Stepped Algorithm for the Treatment of Anxiety Disorders Step 1 Medication Treatment (Usually an SSRI, titrated to a therapeutic dose. If the agent is not tolerated, a second SSRI may be tried.) Cognitive behavior therapy Evaluate response to treatment in step 1. Patients who have a full response to either treatment go to maintenance treatment. Others go to step 2. Step2 Medication treatment Cognitive behavior therapy Partial response Augment anti- depressant or add cognitive behavior therapy No response Cognitive behavior therapy or Different antidepressant type Partial response Augment cognitive behavior therapy (additional sessions) or add first-line antidepressant No response Augment cognitive behavior therapy or add first-line antidepressant Evaluate response to step 2 treatments. Patients with full response go to maintenance treatment. Others are considered for step 3. Step 3 • Consider: • Trial of second or third type of antidepressant (e.g., SNRI, venlafaxine, nefazadone, mirtazapine, and clomipramine) • Intensive cognitive behavior therapy (several times a week) • Other augmentation of antidepressants (if patient had a partial response to an antidepressant in step 2) • Referral to specialty mental health care for more ongoing treatment if more complex problems are present (e.g., childhood abuse and PTSD
Alcohol • TCU Screening • Clinical Assessment • CAGE