Download

1 / 35
350 likes | 450 Views
This document outlines essential strategies for improving healthcare reliability, focusing on effective service delivery through innovative technologies and staff engagement. Key principles include reducing waste, ensuring timely treatments, and creating equitable patient experiences. Through reliable systems, we aim to enhance public confidence in the NHS by minimizing errors and improving patient outcomes. Important metrics for success include reducing length of stay and standardizing care practices, ultimately delivering quality, value, and patient satisfaction.

E N D
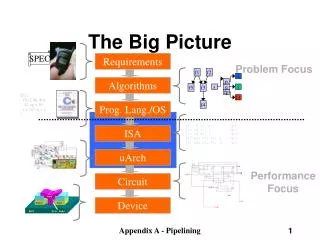
The big picture for improvement: • Making systems more reliable • Linking innovations in service delivery with new technologies • Involving and engaging staff Hugh Rogers Associate, Service Transformation 30th September 2005
Delivering Quality & Value A No Wait system Primary care & LTCs HealthCare Associated Infection The NHS Institute for Innovation and Improvement • NHSU • Leadership Centre • Modernisation Agency • National Innovation Centre
No needless delay Treat me quickly and appropriately No waste Use the resources we give you to greatest effect No feelings of helplessness Treat me with respect and empower me No needless suffering Give me effective treatments and relieve my pain No needless deaths Protect me and heal me No inequity Treat me fairly Adapted from ‘Crossing the Quality Chasm’, Institute of Medicine 2001 The Goal: towards reliable healthcare
What is reliability? • “The capacity to perform a given function under given conditions for a specified period of time” • A reliable health care system is one that is designed to ensure that every patient consistently receives evidence-based, effective care every time he or she needs it. • An important outcome of reliability would be patient and public confidence in the NHS “Reliability means keeping a promise” (Don Berwick)
Measuring reliability (After Nolan & Weick)
Safety Errors of commission special cause strategies reactive focused projects Reliability Errors of omission common cause strategies proactive creation of reliable systems Compare Reliability and Safety When failure has high impact
Current Reliability • Good people working hard will not be able to overcome the complexities of today’s systems of care to prevent errors • Studies show that human beings make errors • Misreading errors 3 in 1000 • Omission in the absence of reminders 1 in 100 (BMJ March 18 2005 Tom Nolan) • NCEPOD report on critical care (May 2005) shows: • 27% of hospitals have no early warning system • 44% of hospitals have no outreach service • 66% of admissions to ICU were unstable for >12hrs (in hospital >24hrs) • 25% were not reviewed by consultant intensivist in first 12 hrs • ICU care ‘less than good’ in 47% • Deficiencies may have contributed to death in 11%
High Impact Changes # 3 #4 and #6 • Manage variation in patient discharge thereby reducing length of stay • Manage variation in the patient admission process • Increase the reliability of therapeutic interventions through a “care bundle” approach
Principles of improved reliability • Understand why LOS varies so much • Benchmarking can help • Variation partly due to variation in clinical care • Establish what care processes need to be standardised to achieve more consistent LOS • Put in place systems whereby this care becomes the default (care bundles) • Establish failsafe mechanisms
Delivering Quality & ValueSystems & Operational Levels OPERATIONAL LEVEL WALK –IN CENTRE DIAGNOSTICS TREATMENT AREAS OPERATING THEATRES PATIENT PATHWAY PATIENT PATHWAY SYSTEM LEVEL PATIENT PATHWAY PATIENT PATHWAY
Focus on improving and standardising core clinical processes Lean principles to reduce waste and apply best practice IMPROVING CLINICAL & SERVICE QUALITY WHILE CONTROLLING COSTS System level • Performance targets • Financial balance • Variation in Practice Operational level • Productivity & efficiency variation • Poor benchmarking
Hip replacement If all trusts moved to perform like the top 10 the NHS would save £48.6 million p.a. • Lower quartile – 10 days • Upper quartile – 8 days • Top 10 performance – 6.3 days
LOS for Fractured Neck of Femur Variation in LOS for different types of hospital • Lower quartile – 19 days • Upper quartile – 13 days • Top 10 performance – 8 days Potential saving £81.4 million p.a.
Stroke Potential saving £74.3 million p.a.
Variation in LOS for Caesarian Section Potential saving £49.1 million
Cumulative % FCEs by HRG 2003/04 for England 100% 90% 80% 70% 60% % All FCEs 50% 40% 30% 20% 10% 0% 1 101 201 301 401 501 601 HRG Source : HES Initial focus for HRGs - episodes 50 HRGs account for 50% of all Finished Consultant Episodes
Admit Admit Admit Presents Presents at A&E at A&E Numbers Numbers A&E A&E Length of stay Length of stay discharged discharged time time How can we improve flow? • Ensure access to a bed • Smooth out elective flow • Expedite simple discharges (across the week and within the day) • Set the discharge date at admission • Patient tracking to record what needs to be done • Make optimum care the default • Standardise care bundles, build in reliability • Maintain decision making throughout the week • Delegation of authority every day • Nurse led discharge • Getting systems right to achieve discharge • Pharmacy, transport, external partners
Defining the optimal clinical process • High volume, high variance clinical groups • Cost, LoS, Staff, Supplies etc. • Study high and low performance • Identify defining characteristics of high performing processes • Field test principles • Design and package for NHS Potential gain for the NHS with the top 50 HRGs: £1,500,000,000 (approx)
Win! Win! Win! Improving and standardising care processes: • Reduces LOS • Reduces staff stress • Improves clinical outcomes • Readmissions • HCAIs But also:
Mortality vs Reference costs Source: ‘Pursuing Perfection’ programme No relationship between cost and mortality
Some specific interventions • Reliability in wards – observations – recognition – responsiveness [hospital at night -> hospital 24/7?] • Critical Care Outreach services and ‘Crucial care’ rounds • Eliminate medical outliers • Eliminate unnecessary delay – access to specialist, higher level care, tests etc • Hospital Infection: ‘Saving Lives’ change package • High risk medications • Decision, planning and diagnostics on admission
May‘04 Blackburn Hospital
Culture for improvement Changing culture • Leadership strategies for openness and mindfulness • Measurement demonstrating change is an improvement • Staff capability – team working – communication up hierarchies
Measuring reliability in Luton • Observations on wards improving • New focus on responsiveness • Testing colour banded EWS and response algorithms • Looking at models of outreach / medical emergency teams • Focus on increase uptake of ALERT training by doctors
The Potential for technology • Frimley Park • Portsmouth • Sydney
3 NHS Trusts, original Community of Practice 295 ‘lives saved’ since April 2004
High Impact Change # 6Increase the reliabilityof therapeutic interventions through a “care bundle” approach • Example for reducing ventilator associated pneumonia: • Elevating the head of the bed >30o (Drakulovic 1999) • DVT prophylaxis (Cook et al 2001) • Peptic ulcer prophylaxis (Yang & Lewis 2003) • Managing sedation effectively with sedation Holds (Kress 2000) • Tight Control of Blood glucose 4.4-6.1 mils (Van den Berghe 2001) • Can be applied to • Surgical site infection • Central line management • Myocardial Infarction • etc etc
Reducing LOS at West MiddlesexGuess when the new hospital opened? New Hospital Opened May 2003
Reducing Mortality at West MiddlesexFrom 1.2 to 0.93 = ~25% New Hospital Opened May 2003
Conclusion By increasing the reliability of clinical care we could: • Save 10,000 Lives per year • Save £1.5 billion per year • The 10 High Impact Changes are just a start • We can only achieve this by changing our organisations and educating our staff