
Enhancing Medication Reconciliation for Patient Safety
This project aims to decrease discrepancies in medication orders to prevent patient harm, by implementing a comprehensive reconciliation process.

Enhancing Medication Reconciliation for Patient Safety
E N D
Presentation Transcript
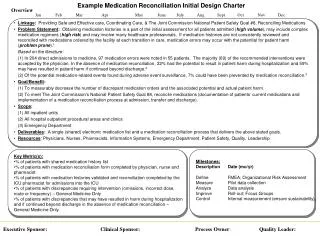
Example Medication Reconciliation Initial Design Charter Overview Jan Feb Mar Apr May June July Aug Sept Oct Nov Dec • Linkage: Providing Safe and Effective care, Coordinating Care, & The Joint Commission National Patient Safety Goal #8, Reconciling Medications • Problem Statement: Obtaining medication histories is a part of the initial assessment for all patients admitted (high volume), may include complex medication regimens (high risk) and may involve many healthcare professionals. If medication histories are not consistently reviewed and reconciled with medications ordered by the facility at each transition in care, medication errors may occur with the potential for patient harm (problem prone).1 Based on the literature: (1) In 204 direct admissions to medicine, 97 medication errors were noted in 55 patients. The majority (69) of the recommended interventions were accepted by the physician. In the absence of medication reconciliation, 22% had the potential to result in patient harm during hospitalization and 59% may have resulted in patient harm if continued beyond discharge.2 (2) Of the potential medication-related events found during adverse event surveillance, 7% could have been prevented by medication reconciliation.3 • Goal/Benefit: (1) To measurably decrease the number of discrepant medication orders and the associated potential and actual patient harm. (2) To meet The Joint Commission’s National Patient Safety Goal #8, reconcile medications (documentation of patients’ current medications and implementation of a medication reconciliation process at admission, transfer and discharge). • Scope: (1) All inpatient units (2) All hospital outpatient procedural areas and clinics (3) Emergency Department • Deliverables: A single (shared) electronic medication list and a medication reconciliation process that delivers the above stated goals. • Resources: Physicians, Nurses, Pharmacists, Information Systems, Emergency Department, Patient Safety, Quality, Leadership Milestones: Description Date (mo/yr) Define FMEA; Organizational Risk Assessment Measure Pilot data collection Analyze Data analysis Improve Roll-out; Focus Groups Control Internal measurement (ensure sustainability) • Key Metric(s): • % of patients with shared medication history list • % of patients with medication reconciliation form completed by physician, nurse and pharmacist • % of patients with medication histories validated and reconciliation completed by the ICU pharmacist for admissions into the ICU • % of patients with discrepancies requiring intervention (omissions, incorrect dose, route or frequency) – General Medicine Only • % of patients with discrepancies that may have resulted in harm during hospitalization and if continued beyond discharge in the absence of medication reconciliation – General Medicine Only Executive Sponsor:Clinical Sponsor:Process Owner: Quality Leader:
References • Scarsi KK, Fotis MA and Noskin GA. Pharmacist participation in medical rounds reduces medication errors. Am J Health-Syst Pharm. 2002; 59:2089-2092. • Gleason KM, Groszek JM, Sullivan C, Rooney D, Barnard C and Noskin GA. Reconciliation of discrepancies in medication histories and admission orders of newly hospitalized patients. Am J Health-Syst Pharm. 2004; 61:1689-1695. • Szekendi MK, Sullivan C, Bobb A, Feinglass J, Rooney D, Barnard C and Noskin GA. Active surveillance using electronic triggers to detect adverse events in hospitalized patients. Qual Saf Health Care 2006; 15:184-190.





















