Download
1 / 48
480 likes | 529 Views
Learn about atherosclerosis, the buildup of fatty plaques in arteries, and its risk factors like dyslipidemia, hypertension, and smoking. Explore the pathogenesis involving endothelial injury and smooth muscle cell proliferation.

E N D
30/4/15 ATHEROSCLEROSIS Dr. Ksheera Cariappa Assistant professor
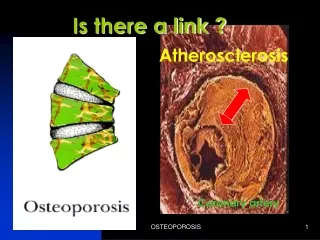
ATHEROSCLEROSIS Definition: Atheroma = porridge. Atherosclerosis is defined as formation of atheromas or atheromatous or fibrofatty plaques in the intima of large and medium sized muscular arteries producing narrowing of the lumen and weakening of the media.
EPIDEMIOLOGY Highest incidence in developed countries. Highest mortality due to IHD. Risk Factors: Major non-modifiable: Age, male sex, family history, genetic abnormalities. Modifiable: Major: Hyperlipidemia, hypertension, diabetes, cigarette smoking. Minor: obesity, alcoholism, infections, homocystinuria, saturated fat intake, sedentary activity, stress – type A personality.
Major Non-Modifiable Risk Factors Age: Dominant influence. Risk increase with each decade. Sex: Males at higher risk of developing atherosclerosis and its complication. Females are protected by estrogen. Familial & Genetic basis: Familial tendency as with familial hypercholesterolemia, hypertension and diabetes; polygenic.
Major Modifiable Risk Factors 1. Dyslipidaemia / Hypercholesterolemia: • Sufficient for the development of atherosclerosis in the absence of other risk factors. • Increased risk with increased levels of LDL (bad cholesterol) that delivers cholesterol to the periphery. • HDL mobilizes cholesterol from atheromas and transports to liver for its excretion in bile. • Higher the levels of HDL lower the risk
Exercise and moderate alcohol intake; increase HDL level. Obesity and smoking decrease HDL levels. High dietary intake of saturated fat; egg yolk, animal fat, butter raises plasma cholesterol. Polyunsaturated vegetable oils; Polyunsaturated fat, omega-3 fat in fish; beneficial
2. Hypertension: Major risk factor. Both systolic (>160mmHg) and diastolic blood pressure (>95mmHg) associated with increased risk. 3. Cigarette smoking: Both in men and women. More the number more is the risk. Cessation; decreases the risk. 4. Diabetes: Induces hypercholesterolemia. Increased predisposition to atherosclerosis.
Multiple risk factors, multiplicative effect. 2 major risk factor = 4 times the risk, 3 major risk factor = 7 times the risk. Atherosclerosis and its complication in an individual in the absence of any apparent risk.
1. Reaction to injury hypothesis • Endothelial injury • Role of blood Monocytes • Intimal smooth muscle cell proliferation • Role of dyslipidaemia • thrombosis
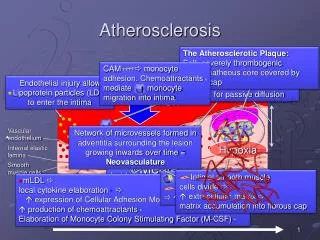
Pathogenesis 1. Role of Endothelial Injury • Chronic and repetitive endothelial injury is the important predisposing factor in the pathogenesis of atherosclerosis. • 2 major risk factors for injury hypertension causing hemodynamic stress & chronic dyslipidaemia • In the absence of endothelial injury, endothelial dysfunction causes increased endothelial permeability and atherogenecity. • Factors that influence endothelial dysfunction are hypoxia, toxins, derivatives of cigarette smoke, homocysteine, infectious agent and cytokines.
2. Role of blood monocytes: • Inflammatory mechanism mediate initiation, progression and complication of atherosclerosis. • In early lesions the endothelial cells express adhesion molecules that binds to leucocytes especially monocytes and T lymphocytes. • Monocytes adhere to endothelium, migrate to intima, transform into macrophages, engulf lipoproteins and transform into foam cells.
3. Intimal smooth muscle cell proliferation: • Platelet aggregation @ site of endothelial injury and monocytes & macrophages release cytokines (IL-1 & TNF-a) causing local synthesis of growth factors (PDGF, FGF & IFN-g, TGF-b) • PDGF & FGF proliferation & migration of SMC’s from media to intima • TGF-b & IFN-g released by activated T-cells regulate collagen synthesis from SMC’s
4. Role of dyslipidaemia: • Mechanism of hyperlipidemia causing atherosclerosis: • Chronic hypercholesterolemia causes endothelial dysfunction by increased production of oxygen free radicals that deactivate NO, endothelial relaxing factor. • Accumulated lipid is oxidized and ingested by macrophages that increase the monocyte accumulation, stimulate CK and GF that are toxic for endothelial cells and ECM.
5. Thrombosis: • Platelet aggregation and smooth muscle proliferation causes mild inflammation which together with the foam cells are incorporated within the atheromatous plaque. • They enlarge by attaching fibrin and cells from the blood & thrombus becomes part of the plaque
2. MONOCLONAL HYPOTHESIS Smooth muscle cells migrate from media to intima, proliferate, deposit extracellular matrix and convert fatty streak into a atheromatous plaque. This theory suggests that SMC proliferation is the primary event & this proliferation is monoclonal as in neoplasms. All SMCs have a single form of G6PD isoenzyme. Initiated by mutations from infections (viruses), chemicals (cigarette smoke), endogenous metabolites(lipids).
1. Fatty Streaks The earliest lesions of atherosclerosis. Composed of lipid filled foam cells. Do not cause any disturbance to the blood flow as the lesions are not significantly raised form the surface. Start as yellow multiple spots less than 2mm and join to form elongated streaks of 1cm or more. In aorta they are seen in all children 10 years or more regardless of any sex, race, geography and environment. In coronary artery starts in adolescence. Precursors of atheromatous plaque.
Distribution: More common in abdominal aorta and the lesions are more prominent around the ostia of the major branches. Order of frequency: Abdominal aorta, coronary arteries, popliteal arteries, internal carotid arteries and vessels of circle of Willis. Vessels of upper extremities are spared. Mesenteric and renal artery ostia.
2. Gelatenous lesions Intima within few months of life Round to oval, grey elevations -1cm Microscopically: foci of increased ground substance in intima with thinned endothelium
3.Atheromatous Plaque: Atheromatous plaque primarily develop in elastic arteries – aorta, carotid and iliac arteries. Large and medium sized muscular arteries – coronary and popliteal arteries. Symptomatic plaques are seen in coronary artery, carotid artery, renal artery, arteries of lower extremities.
Morphology: Atheromatous plaque also called as fibrous, fibrofatty, lipid or fibrolipid plaques. White or whitish yellow. Raised on the surface obstructing the lumen. 0.3 to 1.5 cm but may be larger. Involve only the partial circumference
Morphology: Patchy; along the length of the vessel. With progression; number increases and become diffuse. Consists of; Raised focal lesion. A soft yellow central lipid core. A firm white fibrous cap covering the central core.
Microscopy: Three components: Cells: Smooth muscle cells, macrophages and other leucocytes. Extracellular matrix: Collagen, elastic fibers and proteoglycans. Intracellular and extracellular lipid. Fibrous cap, smooth muscle cells and dense extracellular matrix. Beneath and at the sides of cap (shoulder); macrophages, smooth muscle cells and T lymphocytes. Deep to fibrous cap; central core, composed of necrotic debris, mass of lipid, cholesterol clefts, foam cells and fibrin. Periphery of the lesion; neovascularization
4. Complicated Plaque 1. Calcification deposition in necrotic areas 2. Rupture, ulceration and erosion Atheroemboli: Also called as cholesterol emboli. Discharge of fat debris into the circulation after the rupture of the plaque.
3. Hemorrhage into the plaque: Rupture of fibrous cap or blood vessels; hematoma. 4. Thrombosis: Most dreaded complication. On a disrupted lesion. 5. Aneurysm formation: Due to atrophy of media and loss of elastic fibers; wall weakening and permanent dilatation.
Major Consequences: Myocardial infarction. Cerebrovascular accidents (stroke). Aortic aneurysm. Lower limb gangrene. Mesenteric occlusion
Prevention By risk factor modification. Primary prevention: Aimed to delay the atheroma formation or regressing the established lesions in patients who never suffered serious complications. Secondary prevention: Aimed to prevent the recurrence of complications of atherosclerosis like MI. Cessation of cigarette smoking. Control of hypertension. Weight reduction, Increasing exercise. Moderate alcohol consumption. Lowering total and LDL cholesterol and increasing HDL cholesterol.
COMPLICATIONS PERIPHERAL VASCULAR DISEASE MYOCARDIAL INFARCTION STROKE ANEURYSM FORMATION
COMPLICATIONS Atherosclerotic stenosis • Critical stenosis • Consequences of stenosis Acute plaque change • Stable plaque & vulnerable plaque • Factors that bring about the Change.