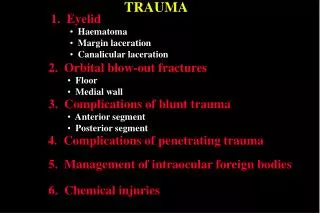
Download
1 / 14
140 likes | 151 Views
Learn about trauma care protocols, the importance of choosing the right hospital, and the factors to consider when making hospital destination decisions in emergency situations.

E N D
SEAEMS TRAUMA FEBRUARY 16,2016
TRAUMA --- • SYSTEM TURNED ON AUGUST 21,2014 • MONTGOMERY 1 LEVEL TWO , 1 LEVEL THREE • DOTHAN 1 LEVEL TWO & 1 LEVEL 3 • REMAINDER OF REGION 10 LEVEL THREE’S AND 3 COMMUNITY HOSPITALS • HOPE FOR COLUMBUS AS TRAUMA • PROJECTED ATS ENTRIES IN SEAEMS 2452 (2479)OR 15 PER 24 HOURS AVERAGE
TRAUMA CHANGES • CALL FROM SCENE BEFORE TRANSPORT BEGUN • CLOSEST HOSPITAL IS NOT ALWAYS THE BEST HOSPITAL • TRANSPORTATION MODE
CALL ATCC EARLY • DIRECTION TO LEAVE SCENE & TRANSPORTATION MODALITY • NOTIFY LAW ENFORCEMENT & FAMILY • TRAUMA TEAM IN WAITING • ONE SCENE IS ONE PIECE OF THE PUZZLE /INTEGRATE FOR RESOURCE USE • PROTOCOL COMPLIANCE
BEST HOSPITAL – TRI-MODAL DEATH • 1/3 @ SCENE • 1/3 FIRST HOUR • 1/3 TWO OR MORE WEEKS POST TRAUMA
BEST HOSPITAL -- SHOCK • FIRST SIGNS OF SHOCK --- AMS & HEART RATE • SHOCK BUILDS DEBT • DEBT MUST BE PAID ,LENGTHENS HOSPITAL STAY ,COMPLICATIONS, DEATH
BEST HOSPITAL SHOCK – INTERVENTION ALS AMBULANCE PREVENTION – HYPOXIA,HEMORRHAGE,CNS INTERVENTION TRANSPORT A SECURE B VENTILATE C CRYSTALOID (2) HOSPITAL • PREVENTION – HYPOXIA,HEMORRHAGE,CNS • INTERVENTION • IMMEDIATE • A SECURE • B VENTILATE • C CRYSTALOID (2)AND BLOOD • D TESTS & SURGICAL INTERVENTION
HOSPITAL COMPARISON Level 3 SURGERY DESIRED ANESTHIA DESIRED X RAY DESIRED RESPIRATORY DESIRED Level 2 • SURGERY REQUIRED • ANESTHIA REQUIRED • X RAY REQUIRED • RESPIRATORY REQUIRED
TRANSPORT BY ALS AMBULANCE IS A FORM OF VERY EFFECTIVE CARE • PHYSIOLOGIC 60 MINUTES OR LESS A LEVEL TWO • ANATOMIC 60 MINUTES OR LESS A LEVEL TWO • ERR ON THE SIDE OF PATIENT CARE • TBI OR AMS LEVEL TWO WITH NS UNDER STROKE RESOURCES • FAMILIES STAY TOGETHER
HOSPITAL DESTINATION DECISIONS • PATIENT (NOT FAMILY ) ALWAYS HAS A RIGHT UNLESS UNDER ARREST • ATCC RECOMMENDS BASED ON REGIONS TRAUMA PLAN AND EMSP ESTIMATE OF TX TIME • RECOMMENDATION NOT BINDING BUT WILL PRODUCE AN ISSUE TO REGION • BINDING IF HOSPITAL IS RED AND NOT PATIENT CHOICE • CLOSEST HOSPITAL IF AIRWAY /BREATHING NOT ABLE TO BE SUPPORTED ,BLEEDING EXTERNAL UNCONTROLLED, BP< 90 NO IV ACCESS. WAIT TO MOVE TO LEVEL TWO
SEAEMS PERFORMANCE • 91 % HOSPITAL OUTCOME REPORTS • 48% EMSP DISCRETION • 27% EMSP ADMIT ( SYSTEM IS 49%) • 13% TRANSFER RATE (ALL ENTRIES ) --- ONE County 23% transfer rate • Level 2’s RED less than one % of time
SUMMARY ISSUES • LIFE IS SAVED BY RIGHT HOSPITAL AS THE FIRST TX DESTINATION • CANNOT ENTER A PATIENT WITHIN 250 FEET OF HOSPITAL • HOSPITALS CAN ENTER PATIENTS • ISSUES WITH ATCC CALL SEAEMS • IF IN DOUBT ERR IN FAVOR OF THE PATIENT. • EMS DESTINATION FOR THE PATIENT NOT EMS CONVENIENCE