Download
1 / 69
690 likes | 807 Views
Primary prevention of SCD using ICD- Review of literature. Dr Frijo Jose A. Risk stratification for ICD therapy. Incidence of SCD in unselected adult population- only 2 per 1000 p/yr Currently, LVEF- 1⁰ factor to select pts for ICD

E N D
Primary prevention of SCD using ICD- Review of literature Dr Frijo Jose A
Risk stratification for ICD therapy • Incidence of SCD in unselected adult population- only 2 per 1000 p/yr • Currently, LVEF- 1⁰ factor to select pts for ICD • SAECG, baseline V arrhythmia, T alternans, autonomic function, EP
Non-invasive evaluation for SCD • Cardiovascular function • h/o syncope • Ventricular arrhythmias • ECG • Autonomic function evaluation • Serum markers • Invasive evaluation of SCD • EPS
Cardiovascular function • LVEF- most consistent & powerful predictor of all-cause & cardiac mortality in IHD & DCMP • NYHA- Despite subjective, imprecise- simple bedside potent risk-stratification tool • Degree of NYHA class- Not linearly related • NYHA classes II & III - much more likely arrhythmia than class IV
Pts with NYHA IV CCF- very ↑mortality from progressive pump failure • Therefore, such pts not usually considered appropriate candidates for ICD therapy • Primary prevention ICD trials have excluded pts with NYHA IV
Pts with syncope have high risk of SCA • In CCF pts with a h/o syncope- incidence of SCD - 45%, V/S incidence 12% in pts with no h/o syncope (p<0.00001) Middlekauffetal. Syncope in advanced heart failure: high risk of sudden death regardless of origin of syncope .J Am CollCardiol 1993;21:110 –116
Ventricular arrhythmias • PVC & NSVT in established SHD- risk marker of SCD- magnitude varies with nature & extent of underlying diseases • IHD- freq & repetitiveness of PVCs, + ↓ LVEF (<30%)- high risk of SCD (Bigger et al- Circulation 1984;69:250–8) • Length but not rate of NSVT- predictor of major arrhythmias in DCM • 3–4 beat runs of NSVT- similar arrhythmia-free survival as pts without NSVT , but incidence of major arrhythmias ↑to 10% per yr in 10 beat runs NSVT (P<0.05). (Grimm et al- Pacing ClinElectrophysiol 2005;28:S207–10)
Standard ECG • Prolonged QRS duration (usually ≥120 ms) and repolarizationabn- independent predictors of SCD • Prolonged QTc(>420 ms, esp long-QT synd) and familial short-QTc (≤300 ms) indicate an ↑risk of SCD
Microvolt T-wave alternans • ABCD trial- • Positive & negative predictive values of MTWA similar to EPS at 1 year • MTWA & EPS have synergistic value • MASTER-I • MTWA did not predict life-threatening ventricular tachyin 575 post-MI with LVEF <30%-but appear to predict all-cause mortality
SAECG • MUSTT -SAECG strong predictor of arrhy death & total mortality • SAECG- excellent - predictive value in IHD, + predictive value is low –limits in preventive therapy • DCM- available data conflicting- • MACAS trial –abn SAECG not helpful for arrhythmic risk prediction. (Grimm et al. Marburg cardiomyopathy study. Circulation 2003;108:2883–91)
Serum markers • BNP might be useful • 521 survivors of AMI- BNP potent predictor even after adjusting for other clinical variables, inclu LVEF. (Tapanainen et al. J Am CollCardiol 2004;43:757–63) • 121 ICD recipients with MI -↑BNP and CRP- asso ↑VT incidence. (Blangy et al. Europace 2007;9:724–9) • BNP is primarily a marker of progressive CHF, which itself may lead to ↑arrhyth- role of BNP- more studies are needed
Invasive evaluation of SCD • IHD- inducibility of sustained V tachy during EPS- well-established marker of SCD • Limitations- • Relatively high number of false-negative- Non-inducibility of VT may not imply a lack of risk • DCM-value of EPS- controversial
Multicenter Automatic Defibrillator Implantation Trial (MADIT, now called MADIT-I)
196 pts- • NYHA- I, II, III with prior MI (≥3/52); LVEF ≤0.35; a documented asymptomatic unsustained VT; and inducible, nonsuppressible VT on EPS • Sustained VT/VF reproducibly induced & not suppressed after IV procainamide • CABG <2/12 or PTCA <3/12 were excluded • ICD (n-95-45+50) V/S conventional medical therapy (n-101) • Death from any cause- end point
Average follow-up- 27/12 • ICD- 15 Ds (11card) V/S Convnt- 39 Ds (27card) • Hazard ratio for overall mortality- 0.46 • Relative risk reduction of 54% with ICD
Subset analysis • Survival benefit from ICD- only in high-risk pts • LVEF <26%, HF requiring therapy, QRS ≥ 120 • Benefit ↑progressively as a function of no of risk factors- greatest reduction in mortality with ICD in those with 2 (HR 0.30) or 3 risk factors (HR 0.20)
MUSTTMulticenter Unsustained Tachycardia TrialBuxton AE. N Engl J Med 1999;341:1882-90 • The trial was designed to study the concept of guiding the management of high risk patients with the results of EPS • Was not primarily designed as a randomized ICD clinical trial
CAD (1/12 - 3yrs) • EF < 0.40 NYHA I,II,III • Asymptomatic nonsustained VT • Primary endpoint: • Arrhythmic death or cardiac arrest • Median follow-up- 39/12
No Rx 7% IA 26% Sotalol 9% ICD 46% Amiodarone 10% MUSTT EP-Guided Rx Patients Treatment at Discharge Antiarrhythmic Drugs: 45% Buxton AE. N Engl J Med 1999;341:1882-90.
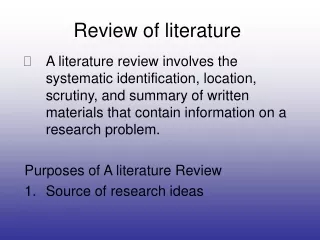
MUSTT Randomized Patient Results Arrhythmic Death or Cardiac Arrest 0.5 No EP-Guided AA Rx EP-Guided Rx, (No ICD and ICD) p = 0.04 0.4 Event Rate 0.3 0.2 0.1 0 0 1 2 3 4 5 Time after Enrollment (Years) Buxton AE. N Engl J Med 1999;341:1882-90.
MUSTT Randomized Patient Results Arrhythmic Death or Cardiac Arrest 0.5 EP-Guided Rx, No ICD No EP-Guided AA Rx EP-Guided Rx, ICD p < 0.001 0.4 Event Rate 0.3 0.2 0.1 0 0 1 2 3 4 5 Time after Enrollment (Years) Buxton AE. N Engl J Med 1999;341:1882-90.
1232 pts with a prior MI (≥1/12) & LVEF ≤0.30 • NYHA-I,II,III • ICD (742) V/S conventional (490) • Invasive EPS not required • End point- Death from any cause
Average follow-up- 20/12 • Mortality rates- • 19.8%- conventional • 14.2%- ICD • HR for risk of any cause death in ICD V/S conventional- 0.69 (P=0.016) • As compared with conventional , ICD asso with 31% reduction in risk of death
At 8 years of follow-up • Cumulative probability of all-cause mortality - 49% among ICD V/S 62% among non-ICD (P0.001) • ICD asso with signi long-term survival benefit (HR- 0.66; P0.001)
Dual-chamber ICDs were programmed to active DDD pacing in MADIT-II regardless of conduction abnormalities as at the time of the study it was hypothesized that AV sequential pacing improves CCF sympts • Dual Chamber and VVI Implantable Defibrillator (DAVID) trial- high frequency of RV pacing with dual-chamber ICD- contributing factor to ↑CCF events & mortality
2521 pts • NYHA class II (70%)or III (30%) & LVEF ≤35% • IHD-52%, DCM-48% • Conventional plus placebo (847) • Conventional plus amiodarone (845) • Conventional plus single-lead ICD (829)
Median follow-up- 45.5/12 • Placebo- 244 deaths (29%), Amio - 240 (28%), ICD- 182 (22%) • Placeb V/S Amio- Similar death risk (HR-1.06;P=0.53) • Placeb V/S ICD- ↓ death risk of 23% (HR-0.77;P=0.007) • Hence, ICD ↓overall mortality by 23% • Results did not vary according to either ischemic or nonischemic causes of CHF
Madit 2- similar • Definite nyha 3 best
Elective CABG-900 -ICD(446) or Control(454) • LVEF <0.36, and abn on SAECG • Average follow- • up of 32/12 • ICD- 101 deaths (71cardiac), Control- 95 (72) • HR for death from any cause- 1.07 (P-0.64)
No evidence of improved survival among CAD pts + ↓LVEF + abn SAECG in whom a ICD was implanted prophylactically at the time of elective CABG
ICD (332) V/S no ICD (342) • 6-40 days after a MI • LVEF ≤0.35 and impaired cardiac autonomic function (↓HR variability or ↑average 24-hr HR on Holter) • mean follow-up -30/12 • No diff in overall mortality betwgps • Although ICD asso with ↓in the rate of death due to arrhythmia, that was offset by ↑in rate of death from nonarrhythmic causes