CPB Problems
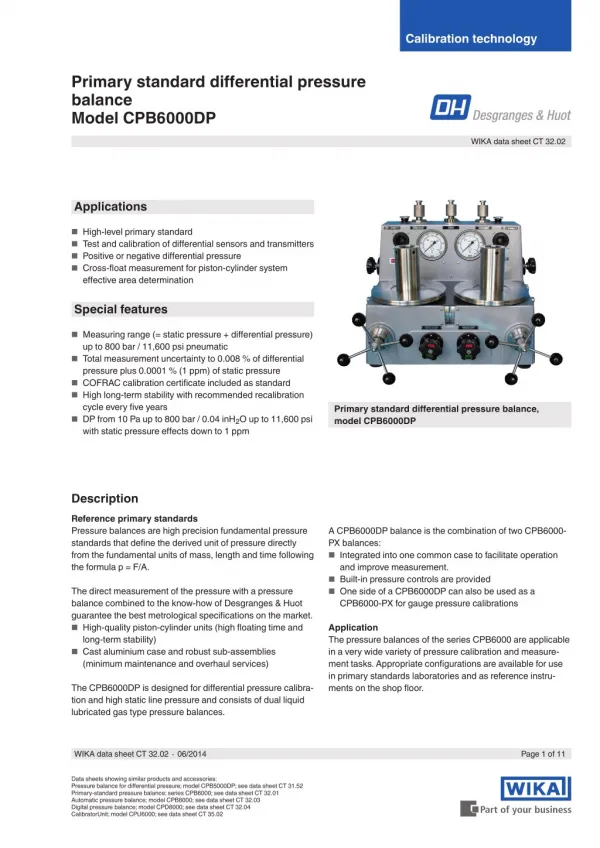
CPB Problems. Mike Poullis. Overview. General Cold Agglutinins Sickle Thalassaemia Hereditary spherocytosis and eliptocytosis Polycythemia G6PD Deficiency Pregnancy SLE VF. In General. If patient warm and well Do CABG off pump Do CPB work warm with blood cardioplegia.

CPB Problems
E N D
Presentation Transcript
CPB Problems Mike Poullis
Overview • General • Cold Agglutinins • Sickle • Thalassaemia • Hereditary spherocytosis and eliptocytosis • Polycythemia • G6PD Deficiency • Pregnancy • SLE • VF
In General • If patient warm and well • Do CABG off pump • Do CPB work warm with blood cardioplegia
Cold Agglutinins 1 • Agglutination and haemolysis of RBC • Cold causes Ab binding • Warm causes complement activation • Screen @ 4oC. If +Ve thermal amplitude test
Cold Agglutinins 2 • Monoclonal lymphoreticular tumours • Polyclonal • Mycoplasma • Glandular fever • CMV
Cold Agglutinins 3 • If polyclonal & elective, cancel and reschedule in 4-6 weeks • Warm CPB and plegia • If cold blood • Warm crystalloid, cold blood, use hot shot • Plasmapheresis, polyclonal Abs, steroids
Sickle 1 • Sickle due to hypoxia, acidosis, infection, capillary stagnation • Homozygous sickle if sats < 85 % • Heterozygous sickle if sats < 40 % • Therefore venous problem • Exchange transfusion, bicarb for venous ABG acidosis, crystalloid or blood(with high Hb A), keep warm • Beware mechanical heart valves causing haemolysis
Thalassaemia • Minor and major • Give blood to make up anaemia • No problems on CPB
Hereditary spherocytosis and eliptocytosis • Increased osmotic and mechanical fragility • Beware mechanical heart valves causing haemolysis • Free haemoglobin possible
Polycythemia • Hct ~70 % • Bleed secondary to [clotting factors] • Autotransfusion good
G6PD Deficiency • 10 to 15% Afro Americans • X linked • Beware sulphonamides, Aspirin, Vit K, ?Sux
Pregnancy 1 • 1st trimester organgenesis, treatogenesis warfarin converted to heparin • 2nd trimester no organogenesis, normal circulation • 3rd trimester hyperdynamic circulation and risk premature labour
Pregnancy 2 • Normal uterine blood flow 1-2 % CO • Pregnant uterine blood flow 10-15 % CO • No autoregulation • Fetal heart rate good monitor • Uterine blood flow reduced by alpha receptors use adrenaline not phenylephrenine
Pregnancy 3 • Keep warm • Use pulsatile • BP > 60 to 70 mean (by flow not alpha blockers) • Hct >22 • Rt flank elevated to reduce caval compression • Tocolytics terbutaline, ritodrine, pregesterone, Mg • Beware serum [k+]
SLE • Lung • interstitial lung disease, PA pressure • Heart • coronary • valve, • conduction • Kidney • renal failure • Blood • Lupus anticoagulant • Neutrophil function with immunosuppression • Brain • encephalopahy • Adrenal • Steroid suppression
VF • Before cross clamp • Cross clamp and pleg • Defib after a few minutes to reduce subendocardial ischaemia • After cross clamp • [k+], lignocaine, suck blood out, Mg2+ • Repleg with warm blood to break reenterant circuit