Download
1 / 19
610 likes | 3.03k Views
Histoplasma capsulatum and Histoplasmosis. Brandon Hang. Outline. Characteristics Pathogenesis Histoplasmosis Pulmonary Disseminated Treatment Future challenges. Characteristics. Member of the phylum Ascomycota Worldwide distribution Naturally found in fecal-contaminated soils

E N D
Histoplasma capsulatum and Histoplasmosis Brandon Hang
Outline • Characteristics • Pathogenesis • Histoplasmosis • Pulmonary • Disseminated • Treatment • Future challenges
Characteristics • Member of the phylum Ascomycota • Worldwide distribution • Naturally found in fecal-contaminated soils • Birds and bats appear to be reservoirs • Etiologic agent of histoplasmosis
Characteristics (cont.) • Dimorphic fungus • Sexual multi-cellular saprophytic mycelia • Asexual single-celled parasitic yeast • Mycelial form is most commonly found in the environment • Heterothallic species • Tightly coiled septate hyphae (A) • Globosecleistothecia (C) • Pear-shaped asci (E) • Smooth, hyaline, spherical ascospores (F) A C E F
Characteristics (cont.) • Yeast form is the infectious agent in humans • Form asexual macro- and microconidia • Also borne by hyphae in the mycelial form (B) • Conidia germinate via non/polar budding • Yeast cells have white, thin-walled, oval bodies (A) A B
Pathogenesis • Infection begins with inhalation of microconidia or hyphal fragments • Mycelial form transforms into yeast form • Triggered by elevated temperatures and increased cysteine levels • 3-stage process • Heat shockphenomenon • Restimulation ofcellular respiration • Increase of RNA& protein synthesis
Pathogenesis (cont.) • Yeast cells are phagocytized by host immune system • M. capsulatum is able to survive phagocytosis • Calcium-binding protein, a cytoplasmic enzyme, a peroxisomal enzyme, and immunogenic M antigen are involved • Apoptosis of infected macrophages allow M. capsulatum to spread • Infection is usually self-limiting in immunocompetentindividuals
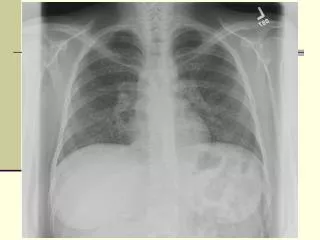
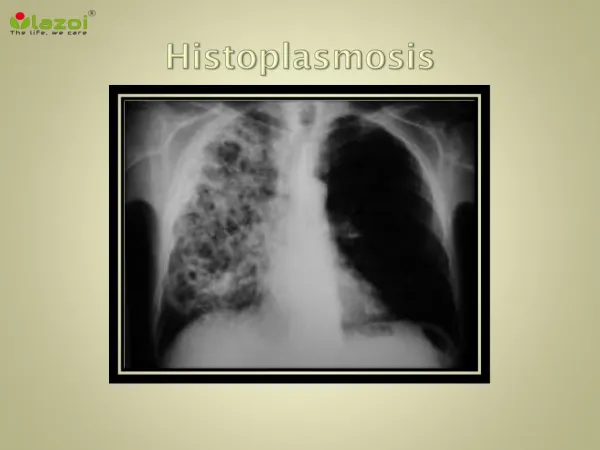
Histoplasmosis • 2 major forms of histoplasmosis • Pulmonary and disseminated • Pulmonary histoplasmosis occurs when microconidia or mycelial fragments are inhaled • Form lesions in the hilar and/or mediastinal nodes • Many types of pulmonary histoplasmosis • Asymptomatic pulmonary histoplasmosis • Acute pulmonary histoplasmosis • Mediastinal granuloma • Fibrosingmediastinitis • Chronic cavitary pulmonary histoplasmosis
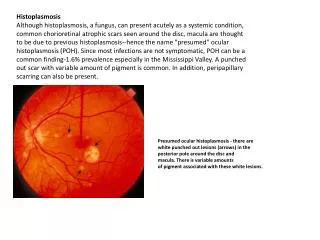
Pulmonary Histoplasmosis • Asymptomatic pulmonary histoplasmosis • Low level exposure to H. capsulatum • 99% of infected people display no symptoms • May display a mild “illness” not recognized as histoplasmosis • Diagnosed using radiography, CT scans, or biopsies
Pulmonary Histoplasmosis (cont.) • Acute pulmonary histoplasmosis • Higher level exposure to H. capsulatum • Patients display fever, malaise, headache, dyspnea, and other respiratory problems • Diagnosed using radiography, BAL, CF, or ID
Pulmonary Histoplasmosis (cont.) • Mediastinal granuloma • Substantial enlargement of a large number of mediastinal lymph nodes • Can impede airways or the superior vena cava • Often matted together and necrotic • Patients have severe chest pain when breathing • Diagnosed using radiography or CT scans
Pulmonary Histoplasmosis (cont.) • Fibrosingmediastinitis • Uncontrolled immune response to necrotizing nodes causes fibrosis around mediastinal lymph nodes • Patients display worsening dyspnea, cough, hemoptysis, and chest pain • Superior vena cava obstruction and heart failure can occur • Diagnosed using radiography and CT scans
Pulmonary Histoplasmosis (cont.) • Chronic cavitary pulmonary histoplasmosis • Exclusive to older patients with emphysema • H. capsulatum infection near emphysematous bullae form a cavity • The cavity progressively grows and spreads from lobe to lobe to form more cavities • Patients display fatigue, fever, anorexia, weight loss, hemoptysis, and dyspnea • Diagnosed using radiography and bronchoscopy
Disseminated Histoplasmosis • Disseminated histoplasmosis • Occurs primarily in immunocompromised individuals • In healthy individuals, H. capsulatum is similar to tuberculosis • While the infection is usually resolved, the fungus is still present • Constantly kept in check by T lymphocytes • In immunocompromised individuals, H. capsulatum is able to spread from the lungs into other organs • Patients display fever, malaise, and occasionally petechiae or skin lesions (cutaneous histoplasmosis) • Tests often reveal mucous membrane ulcerations, simultaneous enlargement of the liver and spleen, and enlarged lymph nodes
Disseminated Histoplasmosis (cont.) • Diagnosis is performed by demonstrating the presence of the fungus in extrapulmonary tissue • Blood cultures, bronchoscopy, BAL, ID, CF, and positive antigen tests are commonly performed • Elevated levels of lactate dehydrogenase and ferritin in AIDS patients
Treatment • Treatment is not required in most cases • Itraconazole and/or amphotericin B in more serious cases • No effective treatment for fibrosingmediastinitis Amphotericin B Itraconazole
Future Challenges • Treatment of fibrosingmediastinitis continues to be difficult and ineffective • Quick and accurate identification of H. capsulatum in infected patients needs to be addressed • Developing a broad spectrum vaccine may be a step in the right direction to address some of these concerns
References Conant, N. F. (1941). Cultural study of the life-cycle of Histoplasma capsulatum Darling 1906. Journal of Bacteriology, 41(5), 563-579. Deacon, J. W. (2005). Fungal biology (4th ed.). Malden, MA: Wiley-Blackwell. Frías De León, M. G., Arenas López, G, Taylor, M. L., Acosta Altamirano, G., & Reyes-Montes, M. del R. (2012). Development of specific sequence-characterized amplified region markers for detecting Histoplasma capsulatum in clinical and environmental samples. Journal of Clinical Microbiology, 50(3), 673-679. Hage, C. A., Wheat, L. J., Loyd, J., Allen, S. D., Blue, D., & Knox, K. S. (2008). Pulmonary histoplasmosis. Seminars in Respiratory and Critical Care Medicine, 29(2), 151-165. Inglis, D. O., Berkes, C. A., Hocking Murray, D. R., & Sil, A. (2010). Conidia but not yeast cells of the fungal pathogen Histoplasma capsulatum trigger a type I interferon innate immune response in murine macrophages. Infection and Immunity, 78(9), 3871-3882. Kauffman, C. A. (2007). Histoplasmosis: A clinical and laboratory update. Clinical Microbiology Reviews, 20(1), 115-132. Keath, E. J., & Abidi, F. E. (1994). Molecular cloning and sequence analysis of yps-3, a yeast-phase-specific gene in the dimorphic fungal pathogen Histoplasma capsulatum. Microbiology, 140(4), 759-767. Khasawneh, F. A., Ahmed, S., & Halloush, R. A. (2013). Progressive disseminated histoplasmosis presenting with cachexia and hypercalcemia. International Journal of General Medicine, 6, 79-83. Kwon-Chung, K. J. (1972). Sexual stage of Histoplasma capsulatum. Science, 175(4019), 326. Maresca, B., & Kobayashi, G. S. (1989). Dimorphism in Histoplasm capsulatum: A model for the study of cell differentiation in pathogenic fungi. Microbiological Reviews, 53(2), 186-209. Newman, S. L., Bucher, C., Rhodes, J., & Bullock, W. E. (1990). Phagocytosis of Histoplasma capsulatum yeasts and microconidia by human cultured macrophages and alveolar macrophages. The Journal of Clinical Investigation, 85(1), 223-230. Pal, J., Ray, A. N., Sherpa, P., Majumdar, B. B., Modak, D., Chatterjee, S., & Sarkar, P. (2013). Primary cutaneous histoplasmosis simulating Molluscumcontagiosum. Journal of the Association of Physicians of India, 61, 498-500. Rossi, S. E., McAdams, H. P., Rosado-de-Christenson, M. L., Franks, T. J., & Galvin, J. R. (2001). Fibrosingmediastinitis. RadioGraphics, 21(3), 736. Sebghati, T. S., Engle, J. T., & Goldman, W. E. (2000). Intracellular parasitism by Hisoplasma capsulatum: Fungal virulence and calcium dependence. Science, 290(5495), 1368-1372. Takahashi, K., Sasaki, T., Nabaa, B., van Beek, E. J., Stanford, W., & Aburano, T. (2012). Pulmonary lymphatic drainage to the mediastinum based on computed tomographic observations of the primary complex of pulmonary histoplasmosis. ActaRadiologica, 53(2), 161-167. Tobón, A. M., Agudelo, C. A., Rosero, D. S., Ochoa, J. E., de Bedout, C., Zuluaga, A., . . . Restrepo, A. (2005). Disseminated histoplasmosis: A comparative study between patients with acquired immunodeficiency syndrome and non-human immunodeficiency virus-infected individuals. The American Journal of Tropical Medicine and Hygiene, 7(3), 576-582. Wheat, L. J., Freifeld, A. G., Kleiman, M. B., Baddley, J. W., McKinsey, D. S., Loyd, J. E., & Kauffman, C. A. (2007). Clinical practice guidelines for the management of patients with histoplasmosis: 2007 update by the infectious diseases society of America. Clinical Infectious Diseases, 45(7), 807-825. Woods, J. P. (2002). Histoplasma capsulatum molecular genetics, pathogenesis, and responsiveness to its environment. Fungal Genetics and Biology, 35(2), 81-97.