Histoplasmosis
Histoplasmosis. By Anastassia Doutova R2 10/06/06. Background. First described by a United States Army physician in Panama in 1906 Histoplasma capsulatum is a dimorphic fungus that remains in a mycelial form at ambient temperatures and grows as yeast at body temperature in mammals.

Histoplasmosis
E N D
Presentation Transcript
Histoplasmosis By Anastassia Doutova R2 10/06/06
Background • First described by a United States Army physician in Panama in 1906 • Histoplasma capsulatum is a dimorphic fungus that remains in a mycelial form at ambient temperatures and grows as yeast at body temperature in mammals. • Endemic to the Ohio, Missouri, and Mississippi River valleys (US) and river valleys between latitudes 45° north and 30° south in North and Central America.
Background Cause • Birds cannot be infected by the fungus and do not transmit the disease but their excretions enrich the growth medium for the mycelium; • bats can become infected, and transmit the fungus through droppings. • Contaminated soil can be potentially infectious for years.
Background Route • inhalation of aerosolized conidia and mycelial fragments from soil results in alveolar deposition • Reactivation can occure • Reinfection is possible although controversial
Epidemiology • Most prevalent endemic mycosis in US • 250-500K individuals are infected annually • 50 million people infected in US • Clinical illness occurs in <5% • in people with underlying lung disease chronic pulmonary histoplasmosis occurs at a rate of 1 per 100,000 persons per year • Clinical symptoms are more frequent in males than in females ratio of 4:1. Except for Rheumatologic manifestations which occur predominantly in females.
Host Response • T lymphocytes are essential in limiting the extent of infection. • Cytokines activate macrophages for fungistatic activity against intracellular yeasts. • Organisms are confined to macrophages • Delayed-type hypersensitivity to histoplasmal antigens occurs 3-6 wk after exposure • 85-90% of immunocompetent individuals produce a positive response to skin antigen test • calcified fibrinous granulomas with areas of caseous necrosis develope over weeks to months.
Course • Can take form of acute or chronic pulmonary infection but may also hematogenously spread systemically • spread may occur through the lymphatics to regional lymph nodes or the liver and spleen. • Progressive disseminated histoplasmosis is rare in adult hosts who are immunocompetent.
PresentationAcute • Most individuals are asymptomatic • Those who develop clinical manifestation - usually immunocompromised - or exposed to a high quantity • onset occurs 3-14 days after exposure
Acute PresentationSymptoms/findings • Common: Fever, headache, malaise, myalgia, abdominal pain, and chills, cough, hemoptysis, dyspnea, chest pain • Large innoculum: severe dyspnea • Uncomon: • Joint pain=arthritis and skin lesions=erythema multiforme, and erythema nodosum (5-6%) mostly in females. • Enlarged hilar and mediastinal lymph nodes are present in 5-10% of patients. • SVC syndrome • Pericarditis In 5% causing cardiac temponade in 40%
PresentationChronic • occurs mostly in patients with underlying pulmonary disease • Reccurent histoplasmosis - latent in healed granulomas
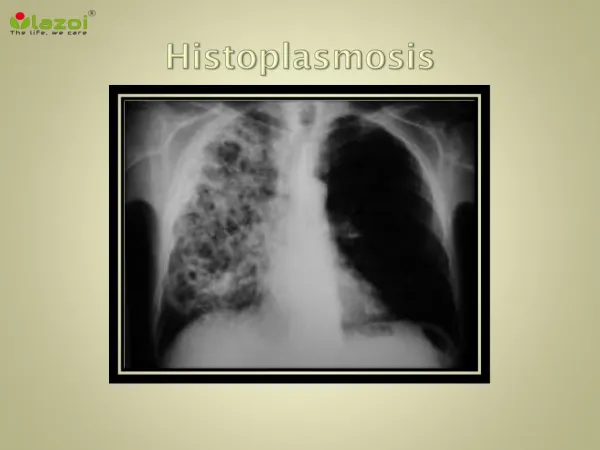
Chronic PresentationSymptoms/findings • cough, weight loss, fevers, and malaise. • ~ 90% of patients develop cavities that may enlarge and result in necrosis. • cavitations may cause hemoptysis, sputum production, and increasing dyspnea • formation of bronchopleural fistulae • Broncholiths • mediastinal granuloma and fibrosing mediastinitis
Presentation Dessiminated Histoplasmosis • Occures in 1 out of 2000 acute cases but in patients with impaired cellular immunity it happens in 4-27% • Can present as subacute, acute or Hyperacute syndrome • typically involves • CNS • liver • spleen • rheumatologic • ocular • Lymphnodes • Mucosal ulcers in 50-60%
Dessiminated HistoplasmosisSymptoms • Subacute/chronic form: constitutional symptoms and • GI: diarrhea and abdominal pain, abdominal mass or intestinal ulcers and lesions, Pancreatitis or cholecystitis • Cards: valvular disease, cardiac insufficiency, vegetations causing dyspnea, edema, angina, and fever. • CNS: headache, visual and gait disturbances, confusion, seizures, altered consciousness, and neck stiffness or pain (meningitis most common) • Other: Hypercalcemia, Mediastinal fibrosis
Accute Dessiminated HistoplasmosisSymptoms • Acute form: generalized symptoms • Severe respiratory distress, DIC, Sepsis • organomegaly • CNS involvement (encephalopathy and meningitis) in 5-20% • Cutaneous lesions in10%
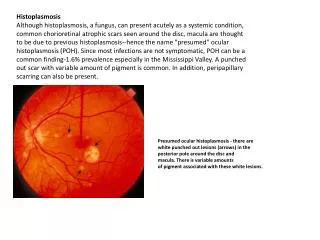
Dessiminated HistoplasmosisOTHER • Ocular histoplasmosis syndrome • Macula involvement may result in blindness • 10% of patients have bilateral involvement • histo spots are Atrophic scars containing foci of lymphocytic cell infiltration
Penumonia Aspergillosis Blasto Carcinoid Lymphoma Ulcerative colitis PCP Sarcoidosis Mycoplasma TB Lung Cancer Chlamedial Pneumonitis Differential diagnosis
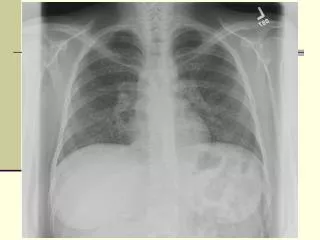
Diagnositc studies • Acute pulm • Sputum cult pos in 10-15% • Fungal Stain (sens 10%) • Complement-fixing Antibodies ( 1:8 exposure, 1:32 active dz) in 5-15% after 3 wks, 95% after 8wks • Anti-M antibody is detected in 50-80% • Anti-H antibody is detected in only 10-20% becomes undetectable in 6m • Serum and urine antigen (sens 25-75%) • Skin test becomes pos only after 1y • CXR: normal, LA, Patchy infiltrates (lower lung fields), reticular nodular or miliary pattern in severe cases
Diagnositc studies • Chronic pulm • Mild anemia • Alk Phosph elevated • Sputum cult pos (sens 50-85%) • Fungal stain (sens 40%) • Complement-fixing Antibodies pos in 70-90% • Anti-M antibody in nearly 100% • Serum and urine antigen (sens 15%) • CXR: Histoplasmomas, Cavitations (upper lobes) in 90%, fibrotic scarring in long-standing cases.
Diagnositc studies • Acute disseminated • Pancytopenia in 70-90% • Blood cult pos in 50-90% • Alk Phosph elevated • Anti-H antibody • Anti-M antibody • Serum and urine antigen (pos in 90%) • CXR hilar lymphadenopathy with diffuse nodular infiltrates in 50% of patients. • Subacute Disseminated • Pancytopenia rarely • Complement-fixing Antibodies pos • CXR has no acute findings • OTHER: PFT’s, Serum angiotensin converting enzyme concentrations , CT (adrenal insufficiency), Bronchoscopy, biopsy
Treatment for symptomatic disease • No treatment for asymptomatic immunocompetent individuals • All chronic histo patients should be treated • Mild forms can be treated with Itraconazole or Ketoconazole PO for 3-6wks • Most cases may require 12-24m course • PO meds effective 75-85%, high relapse rates • Hospitalized Patients should be treated with amphoteracinB IV effective 59-100% given for total of 35 mg/kg • Small cavitary lesions can be monitored, lesions that persist or develop thick walls>3mm should be treated medically /surgically
Treatment for Disseminated disease • Disseminated histo not requiring hospitalization, immunocompetant host - Itraconazole alone 6-18m • Severe dissemintated illness or failure of PO meds can be treated with amphoteracinB IV • Steroids can be used in disseminated histo with respiratory compromise in immunocompetant host (prednisone 60 qd for 2wks) • Patients with AIDS must be on life long therapy • weakly amphoteracinB IV effective 81-97% • Itroconazole effective 90% • Fluconazole effective 88% high relapse
Outcome • Acute pulmonary has excellent prognosis, mediastinal LA resolves over months, rarely diffuse fibrosis occures • Chronic pulmonary Histo can cause cavities that may enlarge and result in necrosis. • Untreated cases may lead to progressive pulmonary fibrosis that results in respiratory and cardiac failure and recurrent infections. • Relapse • chronic pulmonary 20% • acute disseminated 50%, and decreases to 10-20% with life-long antifungal maintenance
Outcome • subacute disseminated • death occurs within 2-24 months in untreated cases • 90% of cases resolve with treatment • Hospitalization frequently required • May be a problem for years with frequent relapse • acute Disseminated • death within weeks if untreated, 50% mortality despite treatment • Almost always requires hospitalization • DIC and sepsis are common • Approximately 5-10% of patients, treated or not, develop adrenal insufficiency • Approximately 10% of individuals develop hyperacute syndrome, which results in death.
Outcome • Reinfection can occur
Summary • Most prevalent endemic mycosis in US • Majority of cases asymptomatic • In immunocompromized host can become disseminated • Diagnostics include serologies, antigen, cultures, radiological findings • All chronic /disseminated cases should be treated • Treatment depends on severity • Great mimicker
Reference • EMedicine • Histoplasmosis Author: Ryan C. Chang M.D. Consulting Staff, Department of Internal Medicine, Divisions of Pulmonary and Critical Care, Kaiser Permanente • UpToDate • Pathogenesis and clinical manifestations of disseminated histoplasmosis • Pathogenesis and clinical manifestations of disseminated histoplasmosis • Pathogenesis and clinical features of pulmonary histoplasmosis