Download
1 / 49
490 likes | 522 Views
Age-related Macular Degeneration (AMD) is an eye disease affecting the macula, leading to central vision loss. Risk factors include age, genetics, smoking, and sunlight exposure. Explore diagnosis, frequency, and treatments for dry and wet forms. Learn about preventive measures and potential hormone treatments like Melatonin. Discover how early detection and monitoring can help manage AMD.

E N D
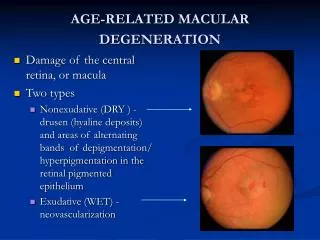
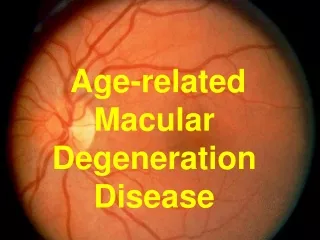
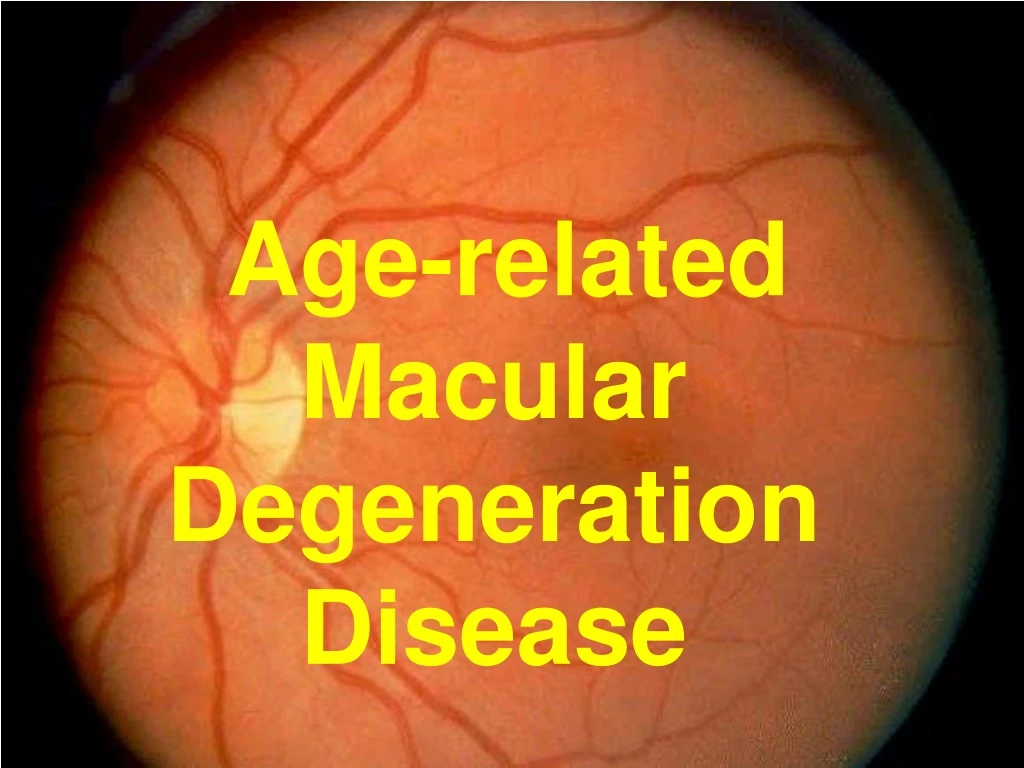
= eye disease that primarily affects the central portion of the retina known as the macula. The risk for developing macular degeneration increases with age and is in excess of 30% by age 75. Age-related macular degeneration The majority of people with macular degeneration have an early form of the condition and experience minimal visual loss. For many of these people, macular degeneration will not progress to a more serious condition. Other risk factors include: a family history of the disease, cigarette smoking, and possibly diet, excessive sunlight exposure, hypertension and cardiovascular disease. Angeles Vision Clinic
Age-related macular degeneration (AMD) How a patient with macular degeneration might see the world. Website
Age-related Macular Degeneration Disease Pathogenesis
Age-related macular degeneration (AMD) Pathogenesis Website
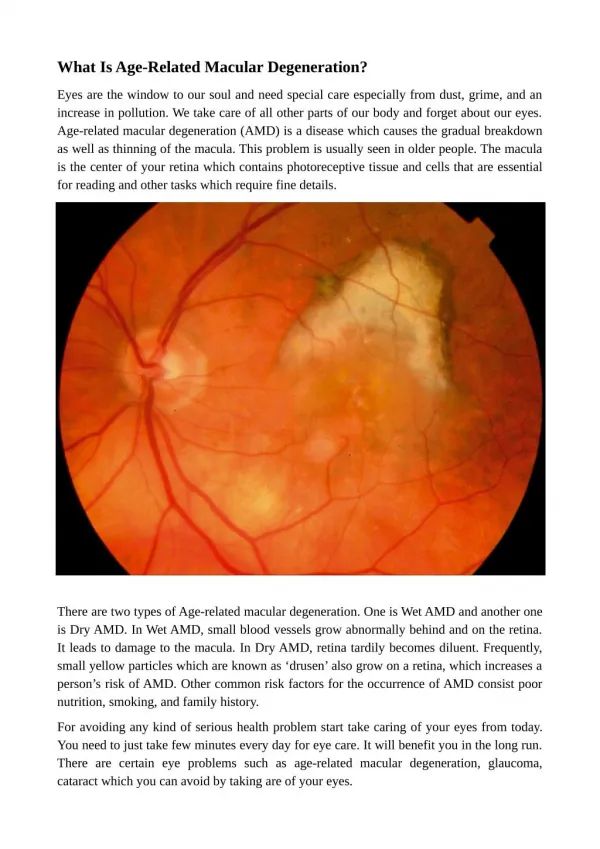
An ophtalmaologist examining a patient at this stage may note the presence of these drusen, even though most people have no symptoms. When drusen have been noted on examination, monitoring will be needed over time, although most patients will not progress to develop visual loss. Many people over the age of 60 will have some drusen. Drusen This retinal photograph shows numerous yellow drusen in & around the macular region of the retina. Angeles Vision Clinic
Age-related Macular Degeneration Disease Diagnosis
Age-related macular degeneration DIAGNOSIS = made based on a thorough eye exam. Eye Exam The doctor looks for presence of abnormalities in the macula, such as deposits called drusen. if the pigmentation is mottled or uneven, instead of its normal even reddish color, macular degeneration is usually the cause. Figure 2. Discrete yellow deposits seen here represent the formation of drusen. Website
Age-related macular degeneration DIAGNOSIS Additional tests are performed to determine the location & extent of the disease: Amsler grid test Fluorescein angiography Indocyanine green angiography (ICGA) Website
Age-related Macular Degeneration Disease Frequency
Dry and wet forms: frequency The dry form represents almost 90% of individuals with ARMD, whereas the wet form is responsible for nearly 90% of severe vision loss.
Dry or atrophic ARMD Dry or atrophic form of age-related macular degeneration (ARMD) = progressive condition that begins with the appearance of drusen in the central retinal area. The dry seen above in fundus photography and in a cross-sectional diagram, = the most common form of macular degeneration, accounting for about 90 % of cases. Although this form of AMD does not usually cause severe vision loss, it can progress to the wet form, so patients who have it should see their ophthalmologist regularly. (Cleveland Clinic)
Wet , exudative macular degeneration = is usually progressive, = experienced as an acute loss of vision or distortion of the objects viewed. Underlying this wet macular degeneration is of new vessel growth from thechoroid, known as choroidal neovascularization, which as a result of exudationof fluid & bleeding into the macula, destroys central vision. Apart from the vitamin supplementation to slow down progression, laser coagulation, photodynamic treatment or vitreoretinal surgery may be helpful in some cases Gandorfer A, Haritoglou C, Priglinger S. [Age-related macular degeneration] MMW Fortschr Med. 2005 May 26;147(21):35-8; quiz 39-40. Operative und konservative Retinologie, Intraokulare Chirurgie, Augenklinik der LMU, Munchen. arnd.gandorfer@med.uni-muenchen.de
Wet ARMD: Macular hemorrhage Note the retinal vessel overlying the hemorrhage. Figure 4. Macular hemorrhage seen in a patient with wet ARMD This finding confirms the hemorrhage seen here is subretinal or choroidal in nature. By Jay M. Haynie, O.D.
What we can we do to prevent, stabilize or slowdown Age-related Macular Degeneration Disease ?
Melatonin The earliest change in the pathologic progression of AMD is the dysfunction of retinal pigment epithelium ( RPE) It was reported that melatonin can control eye pigmentation and thereby regulate the amount of light reaching the photoreceptors disc shedding in cell cultures
Study 1 In vitro: Melatonin protects retinal pigment cells against oxidative stress
Melatonin => protects retinal cells from oxidative stress in vitro Oxidative stress => age-related macular degeneration (AMD). MATERIAL:human retinal pigment epithelial (RPE) cells (ARPE-19 cells) METHOD: cultures => exposed to H(2)O(2) (100 and 200 microm) for 1 hr to induce cell death. Prior to H(2)O(2) treatment, cells => treated w/ various conc. (0.1-200 mcm) of melatonin for 2, 24 or 72 hr. Control cells received either melatonin or ethanol alone. Retinal pigment epithelial cells Liang FQ, Green L, Wang C, Alssadi R, Godley BF. Melatonin protects human retinal pigment epithelial (RPE) cells against oxidative stress. Exp Eye Res. 2004 Jun;78(6):1069-75. Retina Foundation of Sothwest, Dallas, TX 75231, USA. fliang@retinafoundation.org
Melatonin => protects retinal cells from oxidative stress in vitro MATERIAL:human retinal pigment epithelial (RPE) cells RESULTS: SINGLE TREATMENT: 2- & 24-hr pretreatment of melatonin at either conc. => no sign. (P>0.05) protection of cell viability against H202 toxicity PROLONGED TREATMENT w/ MELATONIN (diurnally for 3 days): markedly reduced H(2)O(2)-induced cell death (P>0.05) sign. decreased mitochondrial DNA (mitohchondrial DNA is preferentially susceptible to oxidative damage than nuclear DNA) damage (P<0.05) in RPE cells pretreated vs those without melatonin treatment. CCL: melatonin may protectRPE cells from oxidative stress. Liang FQ, Green L, Wang C, Alssadi R, Godley BF. Melatonin protects human retinal pigment epithelial (RPE) cells against oxidative stress. Exp Eye Res. 2004 Jun;78(6):1069-75. Retina Foundation of Sothwest, Dallas, TX 75231, USA. fliang@retinafoundation.org
Contributing causes to ARMD One of the main mechanism in damaging the RPE in ARMD is throught the accumulation of various free radicals. Melatonin has been demostrated to have the capacity to scavenge the hydroxyl radical Therefore it is reasonable to think that the physíological decrease of melatonin in aged people may be an important factor in dysfunction of retinal pigment epithelial cells
Melatonin Recent studies have also shown that melatonin is related to many eye diseases besides AMD especially in uveitis. There is always some inflammation in the pineal gland in experimental uveitis in the animal model. Further studies involving a bigger randomized sample are needed before its effect can be proven.
Study 2 In vivo in animals: Melatonin protects the eyes of guinea pigs against age-related macular degeneration.
Melatonin => protects the retina against ischemic-reperfusion injury
Study 3 In vivo in humans: Melatonin protects the eyes of patients with age-related macular degeneration
Melatonin => keeps visual acuity stable in patients with macular degeneration
Melatonin => reduces fundus appearance in patients with macular degeneration
A: A 67-year-old male retired teacher. Visual acuity had been decreasing for 2 years B: The same patient with a stable visual acuity at 0.3 with remarkable improvement in subretinal hemorrhage Yi C, Pan X, Yan H, Guo M, Pierpaoli W. Ann N Y Acad Sci. 2005 ;1057:384-92
Female, 71 years old with OD wet AMD, visual acuity improved from 0.2 (A) to 0.4 (B) Yi C, Pan X, Yan H, Guo M, Pierpaoli W. Ann N Y Acad Sci. 2005 ;1057:384-92
Male, 58 years old with OD wet AMD, visual acuity improved from 0.2 (A) to 0.6 (B) one year later. The subretinal hemorrhage and exudate was remarkably absorbed Yi C, Pan X, Yan H, Guo M, Pierpaoli W. Ann N Y Acad Sci. 2005 ;1057:384-92
Man, 65 years old with OD wet AMD, with 0.1 visual acuity with no change after 3 months but fundus improved and macular edema reduced. Yi C, Pan X, Yan H, Guo M, Pierpaoli W. Ann N Y Acad Sci. 2005 ;1057:384-92
Visual acuity improved from 0.2 (A) to 0.3 (B) after 6 month, wet AMD had been largely changed to dry AMD. Subretinal hemorrhage absorbed , some retinal fibrosis developed, the lesion becaame stable. Yi C, Pan X, Yan H, Guo M, Pierpaoli W. Ann N Y Acad Sci. 2005 ;1057:384-92
Melatonin => reduces other opthalmic alterations in patients with macular degeneration PART 1
Melatonin => reduces other opthalmic alterations in patients with macular degeneration PART 2
Women with macular holes => serum GH & IGF-1
GH & Retinal neovascularisation = major cause of untreatable blindness. Numerous clinical reports have postulated a causative role for GH in the pathogenesis of proliferative diabetic retinopathy (1, 2, 3, 4, 5). In addition, increased serum and vitreous insulin-like growth factor I (IGF-I) concentrations have been reported to be associated with proliferative retinopathy (6, 7). Furthermore, IGF-I has been shown to induce angiogenesis in vivo in rabbit cornea and retina models (8). Ischemia-associated retinal neovascularisation was also inhibited in transgenic mice expressing a GH antagonist gene and in normal mice given an inhibitor of GH secretion (MK678) (9). this inhibition could be reversed with exogenous IGF-I administration, transgenic mice expressing the GH agonist E117L had no increase in retinal neovascularisation (9). A decreased prevalence of diabetic retinopathy has also been described in GH-deficient (GHD) diabetics (4, 5), & pituitary ablation has been reported to stop deterioration of visual acuity in patients with diabetic retinopathy (3). Furthermore, continuous infusion of somatostatin has been shown to inhibit development and progression of proliferative retinopathy (10). Blank D, Riedl M, Reitner A, Schnack C, Schernthaner G, Clodi M, Frisch H, Luger A. Growth hormone replacement therapy is not associated with retinal changes. J Clin Endocrinol Metab. 2000 Feb;85(2):634-6. Department of Medicine III, University of Vienna, Austria
Retinal neovaxcularisation • Recently, retinal changes have been reported in two nondiabetic GHD subjects receiving GH replacement therapy (GHRT) over a period of 14 and 22 months, respectively (11). Because symptoms improved or disappeared after cessation of GHRT, a possible causative role for GH has been suggested. Blank D, Riedl M, Reitner A, Schnack C, Schernthaner G, Clodi M, Frisch H, Luger A. Growth hormone replacement therapy is not associated with retinal changes. J Clin Endocrinol Metab. 2000 Feb;85(2):634-6. Department of Medicine III, University of Vienna, Austria
GH => no retinal deterioration 2 cases of retinopathy associated with exogenous GH therapy in nondiabetic patients. Causality by concomitant medications was excluded by a search of the literatureand the FDA data base. The first patient, an obese, 31-yr-old male with traumatic hypothalamic injury, presented with nonproliferative retinopathy & macular edema, resulting in decreased visual acuity (OD 20/40-1; OS countfingers), which required laser surgery. Human GH had been initiated at 0.009 mg/kg.day, 14 months earlier, and titrated to 0.017 mg/kg.day = VERY HIGH DOSES = +/-1.19 mg/day for 70kg The second patient, a nonobese, 11-yr-old girl receiving GH for the management of short stature in Turner's Syndrome, presented with neovascularization. GH doses were 0.033mg/kg.day for the first 17 months and 0.043 mg/ kg.day for the following 5months = VERY HIGH DOSES = +/-1.5mg/day for 35kg Cumulative laboratory and clinical observations suggest that GH andrelated peptides have a role in retinal pathology independent of the degree ofglucose tolerance.Publication Types: Case Reports Koller EA, Green L, Gertner JM, Bost M, Malozowski SN. Retinal changes mimicking diabetic retinopathy in two nondiabetic, growth hormone-treated patients. J Clin Endocrinol Metab. 1998 Jul;83(7):2380-3. U.S. Food and Drug Administration-CDER, Rockville, Maryland 20857, USA.kollere@cder.fda.gov
GH => no retinal deterioration SUBJECTS: 61 GHD patients on GHRT with a mean age of 42.5 yr (+/- 17 yrs) were examined by one ophthalmologist (AR). The mean duration of GHRT was 8.4 yr in childhood onset and 3.5 yr in adult onset patients MEAN DOSE of treatment:1.7 +/- 0.7 IU/day= +/- 0.57 mg/day = high physiological dose RESULTS: In none of the patients could retinal changes like macular edema, microaneurysms, hemorrhages, hard exsudates, cotton wool spots, preproliferative signs, or proliferations be detected in any eye. There was no swelling of the optic disc or vascular abnormality of the optic disc vessels. Blank D, Riedl M, Reitner A, Schnack C, Schernthaner G, Clodi M, Frisch H, Luger A. Growth hormone replacement therapy is not associated with retinal changes. J Clin Endocrinol Metab. 2000 Feb;85(2):634-6. Department of Medicine III, University of Vienna, Austria
HRT = > Eye Ever growing data accumulated over past yrs : HRT: may dry eye symptoms in post-menop. women the intraocular pressure delay cataract formation in treated women. the incidence of aging macular degeneration in post-menop. women. Lang Y, Lang N, Ben-Ami M, Garzozi H. The effects of hormone replacement therapy (HRT) on the human eye : Harefuah. 2002 Mar;141(3):287-91 Dept. of Ophthalmology, Ha'Emek Medical Center, Afula.
HRT => glaucoma
Cost of cataract Jacques PF. The potential preventive effects of vitamins for cataract and age-relatedmacular degeneration. Int J Vitam Nutr Res. 1999 May;69(3):198-205. J.Jean Mayer-USDA Human Nutrition Research Center on Aging, Tufts UniversityBoston, USA. Age-related cataract and age-related macular degeneration (AMD) are importantpublic health problems. Approximately 50% of the 30 to 50 million cases ofblindness worldwide result from unoperated cataract. In the US and otherdeveloped countries AMD is the leading cause of blindness, but age-relatedcataract remains the leading cause of visual disability. Age-related cataractand AMD represent an enormous economic burden. In the United States more than1.3 million cataract extractions are performed annually at a cost ofapproximately $3.5 billion. Much of the experimental research on the etiology ofcataract and AMD has focused on the role of nutritional antioxidants (vitamin C,vitamin E, and carotenoids). Evidence from epidemiologic studies support a rolefor nutritional antioxidants in delaying the onset of these age-related visiondisorders. Although it is not yet possible to conclude that antioxidantnutrients have a role in prevention of cataract or AMD, a summary of theepidemiologic evidence suggests that it is prudent to consume diets high invitamins C and E and carotenoids, particularly the xanthophylls, as insuranceagainst the development of cataract and AMD.Publication Types: Review