Download
1 / 53
780 likes | 1.79k Views
The Controversial Clavicle . G Hansen A Liew Sept 15 th , 2011. Epidemiology. Very common 2.6 – 5 % of all fractures Makes up 3% fractures seen in clinic 71 per 100,000 males 30 per 100,00 females 80% middle third 10-15% lateral third 5% medial third. Anatomy.

E N D
The Controversial Clavicle G Hansen A Liew Sept 15th, 2011
Epidemiology • Very common • 2.6 – 5 % of all fractures • Makes up 3% fractures seen in clinic • 71 per 100,000 males • 30 per 100,00 females • 80% middle third • 10-15% lateral third • 5% medial third
First bone to ossify (5th week fetal life) • Last bone to fuse (medial physis 22-25y) • Only long bone ossify by intramembranous ossification • Medial growth plate makes up 80% growth in length
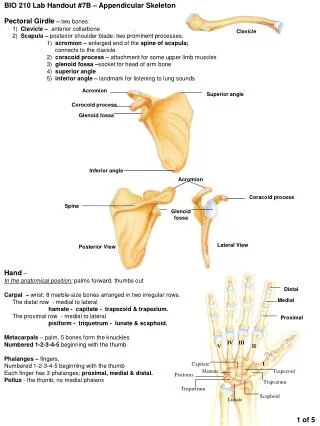
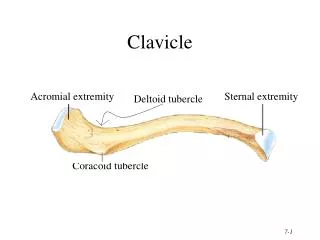
Superior view Inferior view
Function • Acts as a strut to keep shoulder lateral • SC joint is only bony connection of UE to appendicular skeleton • Part of the Superior Shoulder Suspensory Complex
CLAVICULAR FUNCTION 1 2 3 3 Axes of Motion: 1) About the AP axis Elevation & Depression 2) About the Longitudinal axis Protraction & Retraction 3) About the Transverse axis Rotation
CLAVIULAR FUNCTION Protection of underlying N-V structures, i.e., Brachial Plexus, Artery & Vein PLUNGING
MECHANISM OF INJURY DIRECTION OF INJURY • Transitional zone btw outer and middle third • Bone changes from flat to tubular, weakest area • No protective ligamentousattachements
FRACTURE DEFORMITY • Deforming forces uncover 3 potential motions of clavicle • Shoulder droops (depression) • Shoulder adducts (protraction) • +/- rotation • First two ptosis of shoulder • Therefore, medial superior spike is NOT elevated, but results from shoulder drooping FRACTURE
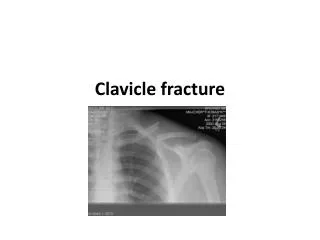
Work Up • Usual Hx and Physical • Open or closed • Careful assessment of NV status • Associated injuries • Sling for comfort
RADIOGRAPHIC ANATOMY In standard AP projection, much of Clavicle overshadowed by other structures In axial (apical lordotic) view, Clavicle seen in better relief
Historic • Neer 1960 – Nonunion of the clavicle. JAMA • 0.1% in 2235 closed midshaft fractures • 4.6% with ORIF • Rowe 1968 – An atlas of anatomy and treatment of clavicle fractures. CORR • 566 midshaft clavicle fractures • 0.8% nonunion with closed treatment • 4.6% nonunion with ORIF
Take home message – that persevered for years to come • Clavicle fracture always heal well • Surgery is difficult with high nonunion rates • Malunion is only of radiographic interest
JBJS(Br) 1997 • n = 242 consecutive clavicle # treated non operatively (sling or figure 8) • 67 completely displaced • 52 followed up average 38 months • 69% satisfied • 8 pts developed nonunion • Initial shortening ≥ 20 mm highly significant association with nonunion • Final shortening ≥ 20mm associated with unsatifactoy result
JOT 2005 • 1975 – 2005 = 22 studies included • Level I: 2 • Level II: 2 • Level III: 4 • Level IV: 14
Conclusions • Meta-analysis of 2144 clavicle fractures: • Nonunion rate of 15.1% with non-op Rx • Associated with displacement, comminution, • Relative risk reduction of 86% for nonunion with ORIF
JBJS 2006 • N = 30 consecutive nonoperative patients • Mean follow up 55months, ROM, Strength, Constant Score, Dash Score
ROM was well maintained • flexion averaging 170° ± 20° and abduction averaging 165° ± 25° • Strength (contralateral limb as control) • Reduced to 81% flexion, 75% endurance of flexion, • 82% abd, 67%endurance abd • 81% ER, 82%endurance ER • 85% IR, 78% endurance IR • Constant score = 71 and Dash score= 24.6 • Substantial residual disability
JBJS 2007 • 132 patients, prospective, randomized • Plate osteosynthesis = 67 • Non operative (sling) = 65 • Inclusion criteria – • completely displaced unilateral midshaft clavicle (no cortical contact btw main two fragments) • Age 16-60 • Middle third of clavicle, not open, no NV injury
Time to union • ORIF – 14.4 weeks • Sling – 28.4 weeks
Conclusion • Early operative fixation of completely displaced midshaft clavicle fractures results in: • Improved patient oriented outcome • Improved surgeon oriented outcome • Earlier return to function • Decreased nonunion rate (2/62 versus 7/49, p=0.04) • Decreased malunion rate (0/62 versus 9/49, p=.01)
JSES 2007 • 2 matched groups • Early and late ORIF (15 pts each) • Early group tested mean 25 months post op • Late ORIF tested mean 33 months post op • Trend towards older age in late group 33 vs 42
Satisfaction • Acute 9.8/10 • Late 9.6/10
Summary • Orthopaedic Clinics North America 2010
Summary • Nonunion rate is 15% • Symptomatic malunion rate is 20% • There are significant residual strength deficits • RCT’s support primary ORIF in selected cases • Delayed reconst. marginally worse then 1˚ ORIF • Scapular winging is a consistent late feature
JPO 2010 • Retrospective review (level III) • 43 consecutive closed midshaft clavicle fractures • Mean age 15.4 y • 25 nonoperative (mean shortening 12.5 mm) • 17 ORIF (mean shortening 27.5 mm) • Union: 8.7 vs 7.4 weeks • Return to activities: 16 vs 12 weeks • Symptomatic malunion 5 non-op (20%) • 4 opted for ORIF with resolution of symptoms
JOT, 2011 • 8 cadavers, 15 clavicles • 3.5mm recon plate with 8 bicortical screws • Each clavicle plated twice, anterior/inferior and superior • Distance screw tip from SV, SA, BP
Conclusions: • Weak study (methodology, small numbers) • However: • Highlights abduction position to minimize risks • Anteroinferior plating is not without consequence
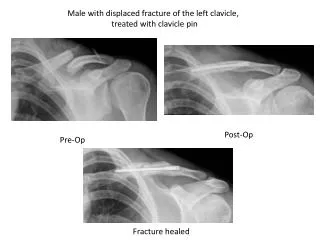
Fixation • Small fragment plates (gold standard) • Precontoured • Locking (? young, good bone) • Reconstruction • Becoming less bulky • Less irritation, less re-operation
Fixation • Intramedullary • Less invasive • Less control (torsion) / reduction • Insertion can be difficult due to sigmoid shape • Further study required • Newer TEN may be promising
Infants • Most common birth fracture • Prevalence btw 0.3 – 3% • >40% not identified until post discharge • Risk factors: • Increased birthweight, prolonged 2nd stage labour, shoulder dystocia, instrumented deliveries • May present as pseudoparalysis, associated with BPP, poor feeding one side, palpable bump, swelling • Morrow (startle) reflex asymmetric • Abundant callus on XR, can be confused with infection • Congenital pseudoarthrosis of the clavicle • Treatment: immobilization by pinning sleeve to shirt
Distal clavicle Anatomy • AC Joint (diarthrodialjt) • Fibrocartilaginous disc • disintegrates by 40yo • Dynamic stabilizers= deltoid and trapezius • Capsule • (prevents 32% posterior clavicle migration) • AC Ligaments (sup/inf/ant/pos) • Mainly horizontal stability • CC Ligaments (Conoid&Trapezoid) • Vertical stability (suspends scapula from clavicle)
Neer Classification • Type I – Distal to CC lig • Minimal displacement due to intact CC lig • Type IIA – Medial to CC lig • Type IIB – Between CC ligs • Type IIA & B – lacks vertical stability of CC lig • Displaced proximal frag, increased non-union • Type III – Intra-articular (AC jt) • CC lig intact, minimal displacement, missed Dx
Imaging • Standard clavicle views • Zanca View • AP view centered at AC joint with 10 degree cephalic tilt • Less voltage than used for AP shoulder • Better appreciation of intra-articular extension • Axillary view for AP displacement • Zanaca
Treatment • Types I and III treated nonoperatively • Both are inherently stable • Due to intact ligaments • Type III may result in AC arthritis, but can be managed with open or arthroscopic distal clavicle excision
Type II • Controversial • High nonunion rates (28 – 44%) if treated nonsurgically • However most “seem” asymptomatic • Sounds familiar?
21 studies, all level III or IV • N = 425 Neer type II fractures • 365 operative • 60 nonoperative • Nonunion: 33% nonop, 1.6% operative • Complications: 6.7% nonop, 22.2% operative • Hook plate highest complication rate (40.7%) • Some inherent • Functional outcomes difficult to assess, but similar btw groups