Download
1 / 30
300 likes | 342 Views
Dive into the causes, types, and treatments of pleural effusion, with insights on diagnosis techniques and various effusion-related conditions such as heart failure, malignancy, and chylothorax. Learn about key indicators and recommended interventions.

E N D
Disorders of the Pleura and Mediastinum Dr. Gerrard Uy
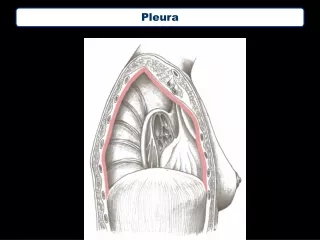
Pleural Effusion • Presence of an excess quantity of fluid in the pleural space • The pleural space lies between the lungs and chest wall and normally contains a very thin layer of fluid
Etiology • Pleural fluid accumulates when pleural fluid formation exceeds absorption • Normally, pleural fluid enters the pleural space from the capillaries in the parietal pleura and removed via the lymphatics
Approach to Patient • Determining the cause is essential • 2 types of effusion • Transudate • Occurs when systemic factors that influence the formation and absorption of pleural fluid are altered • Leading cause: heart failure and cirrhosis • Exudate • Occurs when local factors that influence the formation and absorption of pleural fluid are altered • Leading cause: pneumonia, malignancy, pulmonary embolism
Light’s Criteria • Used to determine the type of pleural fluid • Criteria: • Pleural fluid protein/serum protein > 0.5 • Pleural fluid LDH/serum LDH > 0.6 • Pleural fluid LDH > 2/3 normal upper limit for serum • Misidentify ~25% of transudates as exudates
Effusion Due to Heart Failure • Most common cause of pleural effusion is left ventricular failure • Isolated right sided pleural effusions are more common than left sided pleural effusion • If diagnosis is established, patients are best treated with diuretics • NT pro BNP > 1500 pg/ml is diagnostic of effusion secondary to congestive heart failure
Hepatic Hydrothorax • Occurs in ~5% of patients with cirrhosis and ascites • Direct movement of peritoneal fluid through small openings in the diaphragm into the pleural space • Effusion is usually right sided
Parapneumonic effusion • Most common cause of exudative pleural fluid in the united states • Empyema refers to a grossly purulent effusion • the presence of free pleural fluid can be demonstrated with a lateral decubitus radiograph, CT scan, or ultrasound • If free fluid > 10mm, a therapeutic thoracentesis should be performed
Parapneumonic effusion • Indications for considering CTT insertion • Loculated pleural fluid • Pleural fluid ph<7.2 • Pleural fluid glucose<3.3mmol/L(<60mg/dl) • Positive gram stain or culture of the pleural fluid • Presence of gross pus in the pleural space
Effusion secondary to Malignancy • Secondary to metastatic disease • Second most common type of exudative pleural effusion • Most common tumors causing malignant pleural effusion: • Lung carcinoma • Breast carcinoma • lymphoma
Effusion secondary to Malignancy • Diagnosis is usually made via cytology of the pleural fluid • If cytology is negative, thoracoscopy is the best next procedure if malignancy is highly suspected • If unavailable, needle biopsy of the pleura is the alternative
Mesothelioma • Primary tumors arising from mesothelial cells that line the pleural cavities • Related to asbestos exposure • Thoracoscopy or open pleural biopsy is usually necessary to establish the diagnosis
Chylothorax • Accumulation of chyle in the pleural space • Occurs when the thoracic duct is disrupted • Most common cause is trauma • Thoracentesis reveals a milky fluid with a triglyceride level > 110 gm/dl • Treatment of choice is CTT insertion and administration of octreotide
Hemothorax • Blood in the pleural space • Hematocrite should be obtained from the pleural fluid • True hemothorax if hematocrit is greater than half of the peripheral blood • CTT insertion, thoracoscopy and thoracotomy
Other Causes of pleural effusion • Esophageal rupture • Pancreatitis • Intraabdominal abscess • Meig’s Syndrome – benign ovarian tumor + ascited and pleural effusion
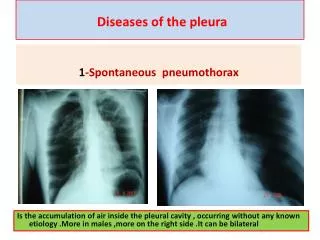
Pneumothorax • Presence of gas in the pleural space • 4 categories • Spontaneous pneumothorax • Secondary pneumothorax • Traumatic pneumothorax • Tension pneumothorax
Spontaneous Pneumothorax • Occurs in the absence of an underlying disease • Usually due to rupture of small apical blebs, small cystic spaces that lie immediately under the visceral pleura • Occurs almost exclusively in smokers • Simple aspiration, thoracoscopy and thoracotomy with stapling of blebs, CTT insertion
Secondary Pneumothorax • Most are due to COPD • Pneumothorax in patients with lung disease are more life threatening than it is in normal individuals • Usually treated with CTT
Traumatic Pneumothorax • Can result from both penetrating or non penetrating chest trauma • Traumatic pneumothorax should be treated with CTT unless very small • Iatrogenic pneumothorax most commonly caused by needle aspiration, thoracentesis and insertion of a central IV catheter
Tension Pneumothorax • Usually occurs during mechanical ventilation or resuscitative efforts • Diagnosis is made by P.E. showing enlarged hemithorax with no breath sounds, hyperresonace to percussion, and shift of the mediastinum to the contralateral side • Treated as a medical emergency • A large bore needle should be inserted at the 2nd anterior ICS
ARDS(Acute Respiratory Distress Syndrome) Dr. Gerrard Uy
ARDS • clinical syndrome of severe dyspnea of rapid onset, hypoxemia, and diffuse pulmonary infiltrates leading to respiratory failure • Caused by diffuse lung injury • The arterial (a) PO2 (in mmHg)/FIO2 (inspiratory O2 fraction) <200 mmHg is characteristic of ARDS • Acute lung injury (ALI) is a less severe form • a PaO2/FiO2 ratio between 200-300 identifies patients who are likely to benefit from aggressive therapy
ARDS • caused by diffuse lung injury from many underlying medical and surgical disorders
ARDS • >80% are caused by severe sepsis syndrome and/or bacterial pneumonia (~40–50%), trauma, multiple transfusions, aspiration of gastric contents, and drug overdose • older age, chronic alcohol abuse, metabolic acidosis, and severity of critical illness
ARDS • Natural history is marked by 3 phases:
Exudative Phase • alveolar capillary endothelial cells and type I pneumocytes (alveolar epithelial cells) are injured • Edema fluid • Cytokines • first 7 days of illness after exposure to a precipitating ARDS risk factor • Dyspnea develops • Chest radiograph reveals alveolar and interstitial opacities involving at least ¾ of the lung fields
Proliferative Phase • lasts from day 7 to day 21 • Most recover rapidly, off ventilation • many still experience dyspnea, tachypnea, and hypoxemia • first signs of resolution • Shift of neutrophil to lymphocytes • proliferation of type II pneumocytes along alveolar basement membranes
Fibrotic Phase • Many patients with ARDS recover lung function 3-4 weeks after the initial pulmonary injury • require long-term support on mechanical ventilators and/or supplemental oxygen • extensive alveolar duct and interstitial fibrosis • emphysema-like changes with large bullae
Treatment • General Principles • (1) the recognition and treatment of the underlying medical and surgical disorders (e.g., sepsis, aspiration, trauma); • (2) minimizing procedures and their complications; • (3) prophylaxis against venous thromboembolism, gastrointestinal bleeding, and central venous catheter infections; • (4) the prompt recognition of nosocomial infections; and • (5) provision of adequate nutrition
Prognosis • Recent mortality estimates for ARDS range from 41-65% • Mortality is largely attributable to nonpulmonary causes • Sepsis and nonpulmonary organ failure account for >80% of deaths • Risk fasctor for mortality includes: • Advance age • Preexsitingmedical condition