Download
1 / 18
190 likes | 788 Views
Diuretics and furosmide. Made by Zainab Albar Supervised by Dr.Ahmad Shaker. Types of diuretics. Loop diuretics ( furosemide , Bumetanide , Torasemide and Ethacrynic acid ). Thiazide (Hydrochlorothiazide , bendroflumethazide or thiazide -like metolazone ).

E N D
Diuretics and furosmide Made by ZainabAlbar Supervised by Dr.Ahmad Shaker
Types of diuretics • Loop diuretics ( furosemide , Bumetanide , Torasemide and Ethacrynic acid ). • Thiazide(Hydrochlorothiazide ,bendroflumethazide or thiazide-like metolazone). • Potassium sparing diuretics : Aldosteroneanatgonist as (spironolactone , canrenoate and eplerenone ) and sodium channel blocker (amiloride and Triamterene) • Carbonic anhydrase inhibitor ( Acetazolamide, Dorzolamide and methazolamide ) . • Osmotic diuretics ( Mannitol ) .
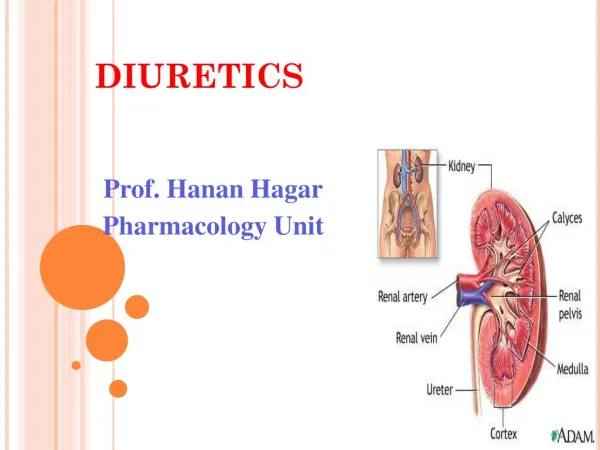
Furosemide • Mechanism of action : inhibits reabsorption of NaCl in ALH and DCT . Increase excretion of Na,Cl,Mg and Ca. • pharmacodynamics/kinetics : • Onset of Action : oral , S.L. : 30-60 MIN . • I.V. : ~ 5 MIN, Bioavailability ~ 100 % • Peak effect : oral, S.L : 1-2 hrs. • Duration : oral, S.L : 6-8 hrs, I.V. : 2 hrs. • Protien binding : 91 to 99 % to albumin. • Half life elimination : with NL Renal function 0.5-2 hrs., ESRD ~ 9 hrs. • Excretion : Urine ( oral 50 %, I.V. 80 % ) within 24 hrs .
Dosage : • Oral : 20 – 80 mg/dose , with increment increase 20 – 40 mg/dose at interval 6-8 hrs up to max 600 mg / day . • IV : 20-40 mg/dose , once or twice daily . Max per dose is 200 mg . • Infusion : 10-40 mg/hr if uop less than 1 mg/kg/hr double as necessary to max 80-160 mg/kg/hr.
Contraindication • Hypersensitivity to sulfonamides. • Pregnancy RISK FACTOR CLASSS C . • Adverse reaction : • Hyopkalemia • Alkalosis • Hypocalcemia • Hypomagneseima • Hyperuracemia • Ototoxcicity. • Drug interactions : • Amioglycosides enhanced otoxocicity. • Lithium ( decrease clearnce with chronic use of loop diuretics) • Digoxin ( increased toxocicity with electrolyte distubance)
Why we do not rely on oral fruosemide in management of acute pulmonary edema ?
Oral fruosemide has very variable bioavailability ranging from 20 to 64 % . And it has been claimed that the absorption and effectiveness of fruosemide is diminished in patients with HF due to edema of the bowel and decreased splanchnic blood flow . 5,8,9 Oral Bioavailability in HF varies widely (34 -80%).
One might prefer IV route gives a better response . Surprisingly ! this is not always the case . In both healthy volunteers and patients with HF , total daily fluid and electrolytes loss after oral therapy and parenteral therapy are comparable . The major difference is in TIME COURSE OF RESPONSE .5,6,7 Note : we avoid using oral in acute setting ONLY for variable bioavailability and slower action than IV .
INFUSION VS BOLUSES • Theoretically in view of PK principle , in infusion we get rapid response with less fluctuation in blood level and in diuretic response plus fewer adverse effects .4 • meta-analysis in 2012 showed statistical support for administering furosemide as a continuous infusion for greater diuresis and reduction in total body weight in patients hospitalized with ADHF. But Larger studies are needed to provide robust recommendations for clinical practice. 2 • In DOSE trail 2010 , there was no statistically significance difference between continuous infusion or twice daily bolus injection in term of global assessment of symptoms , change in creatinine ,net fluid loss ,change in weight or length of hospital stay . 3
Summary • The evidence base for use of diuretics is limited. However, their use as first line management in HF is firmly established in clinical practice and endorsed in clinical guildlines as class (1) recommendation .1, • Infusion is better than bolus in term of diuresis , lower dosage , less toxicity( from Pk view ) . But no significant difference in term of global assessment of patient . • Better to use IV either infusion or injection in acute HF for faster relive of symptoms.
PROMIZING STUDIES • USE OF DOPAMINE TO ASSISST DIURESIS AND PRESERVE RENAL FUNCTION BUT TRAILS ARE UNDERWAY TO CONFIRM CLINICAL VALUE OF THIS AGENT .1, • WE NEED TO MAKE INVESTIGATEION TO ESTIMATE PHARMACOKINATICS ( LD & INFUSION RATE ) TO REACH OPTIMAL DOSE ON SAUDI POPULATION .
References • 1 The use of diuretics in acute heart failure :evidence based therapy ? Ali Vazir, Martin R. Cowie. Cardiology Royal Brompton hospital , UK.2013,April. • 2 Continuous infusion versus intermittent bolus furosemide in ADHF: an updated meta-analysis of randomized control trials. 2012 Mar,Amer M, Adomaityte J, Qayyum R. Division of General Internal Medicine/Hospitalist Program, Johns Hopkins School of Medicine, Baltimore, MD, USA. mamer1@jhmi.edu • 3 Allen, L.A., Turer,A.T., Dewald T., Stough, W.G., Gotter, G. and O’connor, C.M. 2010 continous infusion vs bolus dosing of fruosemide for patient hospitalized for heart failure, american journal of cardiology . • 4 Continuous infusion of loop diuretics in the critically ill: a review of the literature. • Martin SJ, Danziger LH. Source:Department of Pharmacy Practice, University of Illinois at Chicago 60612. Crit Care Med. 1994 Aug;22(8):1323-9. Review. • 5 Greither A et al , pk of fruosemide in patients with CHF, 1979;19;121. • 6 Kelly M et al . A comparison of the diuretic response to oral and IV fruosemide in diuretic resistant patient s Curr The Res 1977;21;1. 7- 94 • 8Brater DC Pharmacology of diuretics AmJ Med Sci 2000,319,:38 • 9Kramer BK et al .Diuretic traetment and resistance in HF ,AmJ Med 1990,106;90. • 10 Meir Lahav,MD, ArieRegev, MD, Pra R aanani,MD and Emanuel Theodor,MD .Intermittent adminestration of fruosemidevscontinous infusion preceded by a loading dose for congestive HF . 1992,SEP. • 11 applied therapeutics , the clinical use of drugs 8th edition . Mary Anne Koda Kimble ROBIN l . Corelli. • 12 KAPLAN PHARMACOLOGY EDITION 2013, 13 www.drugs,com.