Diuretics
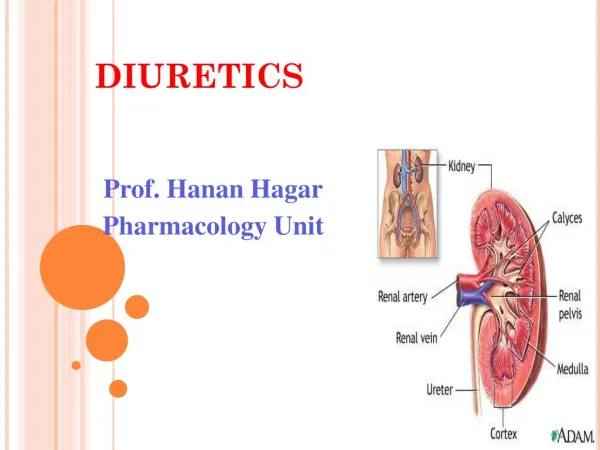
Diuretics. Remove sodium & water tx hypertension, CHF, pulmonary edema, kidney disease nursing diagnosis - fluid volume excess. Renal Physiology. Urine formation occurs in nephron where blood plasma is processed into urine


Diuretics
E N D
Presentation Transcript
Diuretics • Remove sodium & water • tx hypertension, CHF, pulmonary edema, kidney disease • nursing diagnosis - fluid volume excess
Renal Physiology • Urine formation occurs in nephron where blood plasma is processed into urine • ADH – released when osmolality of extracellular fluid increases which increases water reabsoprtion • Acid-base regulation • Usual urine production is less than 2L/day
Carbonic Anhydrase Inhibitor • Enzyme (carbonic anhydrase) acts to promote reabsorption of sodium and bicarbonate • Diamox (acetazolamide) • Agents used more for glaucoma than as diuretic • may cause false positive urine protein test • take with meals
Loop Diuretics • Inhibit reabsorption of sodium and chloride in the ascending loop of Henle • effective even with impaired GFR • watch for hypokalemia • Lasix (furosemide) - may raise glucose level, push slowly with IV, store oral solution in refrigerator
Osmotic Diuretics • These agents are filtered by glomerulus but have limited capability of being reabsorbed • Used primarily with increased intracranial pressure but also may be used with ARF • mannitol (Osmitrol) - IV, if crystals form, warm sol. then cool to body temp., IV set must have filter, infiltration may result in tissue necrosis
Thiazide Diuretics • Safest diuretic • Structurally related to antibacterial sulfonamides • inhibit sodium and chloride reabsorption in early portion of distal tubule • watch for hypokalmia • adverse effects - hyperglycemia and hyperuricemia) • HydroDIURIL (hydrochlorothiazide)
Potassium-sparing Diuretics • The drugs in this class have different modes of action • Dyrenium (triamterene) & Midamor (amloride) blocks sodium reabsorption in distal tubule • Aldactone (spironolactone) - inhibits action of aldosterone, adverse effect is gynecomastia for male clients • Generally used with potassium-depleting diuretic
Combination Diuretics • Combines potassium sparing diuretic with hydrochlorothiazide (HCTZ) (thiazide diuretic) • Aldactozide (spirolactone & HCTZ)
Nursing Implications • Monitor I&O, weights • Monitor potassium, chloride, glucose, uric acid • Give early in day • Watch for Digoxin toxicity for clients on Digoxin
Critical Thinking Ms. Jones is admitted with CHF. She is started on HydroDIURIL. What type of diuretic is this? What lab data would you check prior to giving this medication? What are the adverse effects you will be monitoring for? What do you expect to see if Ms. Jones has a therapeutic response?
Critical Thinking (cont) Ms. Jones is having difficulty breathing. The physician orders Lasix IV. Is impaired renal function a contraindication? What primary electrolyte imbalance will you monitor for? What precautions will you take when administering Lasix IV?