Download
1 / 46
500 likes | 652 Views
Learn about the structure of the alimentary canal from mouth to anus, functions of the digestive system, and common disorders like dysphagia, gastritis, and peptic ulcers. Explore causes, symptoms, and risk factors in detail.

E N D
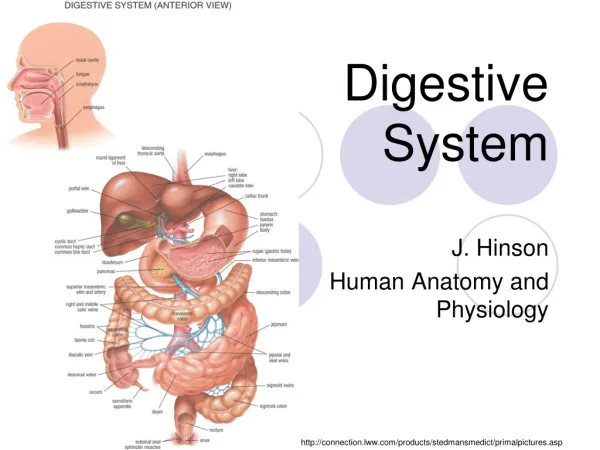
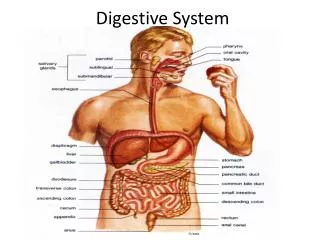
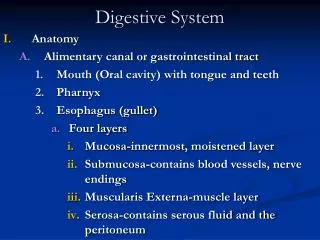
Structure of alimentary canal • Extending from mouth to anus. • Is about 4.5-6 meters in length. • It consists of: 1-Mouth 2-Oral Cavity 3-Pharynx 4-Esophagus 5-Stomach 6-Small intestine: Duodenum, Jejunum and ileum 7-Large intestine: 9-Anal canal
Accessory structures • Not in tube path • Organs • Teeth • Tongue • Salivary glands • Liver • Gall bladder • Pancreas
Functions of The Digestive System 4 Functions: 1- Motility 2- Secretion 3- Digestion 4- Absorption
General Symptoms of GI diseases 1-Anorexia : loss of appetite 2-Nausea 3-Vomiting 4-Diarrhea , constipation 5-Abdominal pain: which may be burning, dull aching or colicky (means gradually becoming worse, then easing off again.) 6-Bleeding: obvious or occult 7- Heartburn 8- Indigestion, bloating
Dysphagia • Difficulty swallowing. • It is usually a sign of a problem with throat or esophagus,( the muscular tube that moves food and liquids from the back of mouth to stomach Risk factors • Aging. • Certain health conditions. People with certain neurological or nervous system disorders are more likely to experience difficulty swallowing.
Symptoms • Having pain while swallowing • Being unable to swallow • Having the sensation of food getting stuck in your throat or chest or behind your breastbone (sternum) • Drooling • Coughing when swallowing
Causes: • There are two types of problems : • * Impaired motility of esophageal wall (the muscles and nerves that help move food through the throat and esophagus are not working right) caused by neurologic disorders: e.g. brain injury, stroke or parkinson’s disease • *Something is blocking throat or esophagus (esophageal obstruction), this may happen in case of tumors
Gastritis • Gastritis means inflammation of the gastric mucosa. • Gastritis may occur suddenly (acute gastritis), or it can occur slowly over time (chronic gastritis). Weaknesses in the mucus-lined barrier that protects stomach wall allow digestive juices to damage and inflame stomach lining.
What Are the Symptoms of Gastritis? • upper abdominal pain • indigestion or bloating • nausea and vomiting • belching • loss of appetite or weight loss In more extreme cases, you may experience stomach bleeding and/or black stools
Causes of Gastritis • Long-term use of certain medications (aspirin) • Excessive alcohol consumption • Bacteria that cause stomach ulcers (H. pylori) • Certain illnesses (kidney failure) • A viral infection in a weakened immune system • Persistent, intense stress
1- Acute Gastritis • Acute gastritis refers to a transient inflammation of the gastric mucosa. • It is most commonly associated with local irritants such as bacterial endotoxins, alcohol, and aspirin.
2- Chronic Gastritis • Involves swelling or inflammation of the stomach lining • There are three major types of chronic gastritis: • Type A is caused by immune system destroying stomach cells. • Type B, the most common type, is caused by Helicobacter • pylori bacteria, and can cause stomach ulcers, intestinal ulcers, and cancer. • Type C is caused by chemical irritants like alcohol.
Complications of chronic gastritis • Gastric atrophy 2. Achlorhydria: it means that stomach fails to secret hydrochloric acid. 3. Pernicious anemia: the loss of the stomach to secret intrinsic factor will cause the loss of the ability to absorbed vitamin B12. Vitamin B12 is needed for normal production of RBC this is why its deficiency causes Pernicious anemia.
Peptic ulcer • Is an open sores that develop on the inside lining of stomach and the upper portion of small intestine caused by the digestive action of gastric juice. Peptic ulcers include: Gastric ulcers that occur on the inside of the stomach Duodenal ulcers that occur on the inside of the upper portion of small intestine (duodenum)
Site : • - First few centimeters of the duodenum (most frequent site). • - Along the lesser curvature of antral region • - Lower end of esophagus (rare).
Pathophysiology of peptic ulcer • The basic cause of peptic ulcer is too much secretion of gastric juice in relation to the degree of protection by gastroduodenal mucosal barrier • So, peptic ulcers are caused by A. Excess secretion of acid and pepsin by gastric mucosa. B. Decreased capability of gastroduodenal mucosal barrier to protect against the digestive action of acid-pepsin complex. e.g, 1-Stress ,2. Alcohols ,3. Aspirin. 4. Salts and sugars of high concentrations.
Peptic Ulcer (contin) • Manifestations: 1- Burning stomach pain 2-GI bleeding 3- The vomiting of blood — which may appear red or black 4- Dark blood in stools or stools that are black 5- Nausea or vomiting • Treatment: 1-Avoidance of smoking 2-Antibiotics to treat H.pylori 3-Antacids that neutralize stomach acid 4- Medications that block acid production (Proton pump) inhibitors reduce stomach acid 5-Surgical Treatment : used when medical treatment fails.
Intestine: irritable bowel syndrome • One of the most common GI disorders that affects the large intestine (colon). • Symptoms: 1-GI pain 2-Gas bloating 3-Altered bowel functions: diarrhea or constipation • Cause: hypereactivity of the bowels.
It doesn't cause changes in bowel tissue or increase risk of colorectal cancer. Only a small number of people with irritable bowel syndrome have severe signs and symptoms. Some people can control their symptoms by managing diet, lifestyle and stress. Others will need medication and counseling
Causes It's not known exactly what causes irritable bowel syndrome, but a variety of factors play a role. The walls of the intestines are lined with layers of muscle that contract and relax in a coordinated rhythm If you have irritable bowel syndrome, the contractions may be stronger and last longer than normal, causing gas, bloating and diarrhea. Or the opposite may occur, with weak intestinal contractions slowing food passage and leading to hard, dry stools.
Common triggers include Foods Stress Hormones Other illnesses • Treatment: • 1-Tranquilizers • 2-Dietary: increased fiber consumption • 3-Symptomatic treatment as antidiarrhea and antispasmodic
Gall bladder • Gall bladder is a sac-like structure that stores bile formed in the liver • At time of meal its wall contract , so bile passes to the duodenum • In the duodenum, bile salts cause fat digestion and absorption • Bile is composed of : water, bile salts, cholesterol and bile pigments (bilirubin)
Gall stone formation (Cholelithiasis) • Is the most common disorder in digestive system • Predisposing factors: • 1- Aging • 2- Excess cholesterol • 3- Obesity • 4- Abnormal fat metabolism
Gall stone formation (Cholelithiasis) Types of gallstones •Cholesterol gallstones. Is the most common type of gallstone, often appears yellow in color. These gallstones are composed mainly of undissolved cholesterol, but may contain other components. •Pigment gallstones. These dark brown or black stones form. They're made up of bilirubin • Manifestations: 1- Acute and severe abdominal pain 2- Nausea, vomiting, fever and chills 3- Jaundice if obstruction occurs • Diagnosis: 1- Radiography 2- Ultrasonography 3- Cholecystoscopy
Gall stone formation (contin) • Treatment: 1- Surgical removal of gall bladder (Cholecystectomy) 2- Endoscopic removal of gall stones 3-Lithotripsy: use of ultrasound waves to break up the gall stones 4- Low fat diet • N.B. Cholecystitis: is an acute or chronic inflammation of gall bladder. Most commonly caused by the presence of gall stones. Treatment like that of gall stone formation.
Liver: Functions 1- Carbohydrate, fat and protein metabolism 2- Metabolism of steroid and sex hormones 3- Formation of bile and elimination of bilirubin 4- Synthesis of plasma proteins and clotting factors 5- Storage of glycogen, minerals and vitamins 6- Drug metabolism
Liver: Hepatitis • Definition: means inflammation and possible injury of the liver. • Causes: 1- Viruses (most important) 2- Alcohol 3- Toxins 4- Drugs
Viral Hepatitis • Means inflammation of the liver caused by viral infection. • Hepatitis viruses include: A,B,C,D and E • All hepatitis viruses target the liver cells as their site of infection and replication • Manifestations of viral hepatitis: 1-Range from asymptomatic to severe 2-Fatigue, malaise, anorexia and nausea 3-Jaundice 4-Liver inflammation and abdominal pain 5-Abnormal liver functions and enzyme levels.
Hepatitis B This type is transmitted through Sexual contact. Sharing of needles. Accidental needle sticks. Mother to child Hepatitis A This type of hepatitis is most commonly transmitted by consuming food or water contaminated by feces from a person infected with hepatitis Being in close contact with a person who's infected —
Hepatitis C is transmitted through direct contact with infected body fluids, typically through injection drug use and sexual contact Hepatitis D HDV is contracted through puncture wounds or contact with infected blood
Treatment of hepatitis • Many hepatitis infections will resolve within 4-8 weeks without treatment. The long- term course of hepatitis B and C make it less predictable. • Alpha interferon (IM or SC) is used for both treatment of chronic hepatitis B and C. • IV glucose administration if oral intake is inadequate. • Avoidance of active exercise.
Cirrhosis • Cirrhosis is characterized by diffuse scarring and fibrosis of the liver in response to chronic inflammation and injury. • Manifestations of liver cirrhosis: 1- Hepatosplenomegaly 2- Portal hypertension is (an increase in the blood pressure within a system of veins called the portal venous system) 3- Ascites 4- Edema 5- Esophageal varices(enlarged veins in the lower part of the esophagus ) and hematemesis (the vomiting of blood) 6- Liver failure 7- Jaundice 8- Hepatic encephalopathy 9- Hepatorenalsyndrome
Treatment of liver cirrhosis 1-Nutritional and vitamin supplementation. Reduced-protein diet is useful to decrease ammonia 2- Diuretics to relieve fluid accumulation 3-Management of symptoms
Formation of bile pigments • Old red blood cells become too fragile to exist in the circulatory system. Their cell membrane rupture and the released hemoglobin is phagocytosed by the reticuloendothelial system (REs). Here, the hemoglobin splits into globin and heme and the heme ring is opened to give a) Free iron that is transported in the blood by transferrin, b) Bilivirdin, the first bile pigment which is rapidly reduced to bilirubin which is gradually released from RES into the plasma. • The free bilirubin immediately combines strongly with plasma albumin to form hemebilirubin, free or unconjugatedbilirubin.
Formation of bile pigments • Within hours, the bilirubin is absorbed through the hepatic cell membrane, leaving the plasma albumin. • Inside the liver cells, bilirubin is conjugated with either glucuronic acid or sulphateto form conjugated bilirubin (cholebilirubin) • In the intestine, the conjugated bilirubin (cholebilirubin) is converted by bacterial action to urobilinogen where, - 25% is reabsorbed by the intestine to the liver. 20% is resecreted by the liver back into the gut and 5% is excreted in the urine. After exposure of the urine to air, urobilinogen is oxidized into urobilin. - 75% is converted to stercobilinogen. After exposure of feces to air stercobilingen is oxidised to stercobilin that causes the normal brownish colour of the stools.
Jaundice • Definition : yellowish colouration of the skin and mucous membranes due to increased concentration of total bilirubin in the blood (hyperbilirubinemia). Normally, total bilirubin (free and conjugated) is 0.5 mg/dl. Jaundice appears when the concentration of total bilirubin in blood rises above 1.5 mg/dl.
Causes and Types of jaundice 1. Hemolytic (prehepatic) jaundice : - Caused by increased destruction of RBCs (hemolysis) • The rate of formation and excretion of bilirubin is increased, however, the rate of formation exceeds the rate of hepatic uptake. • 2. Obstructive or cholestatic (post'hepatic) jaundice : • Caused by obstruction of the biliary passages. 3. Hepatogenous (Hepatic) Jaundice - Caused by damage of the liver cells mainly as a result of viral hepatitis. • The diseased liver cells are unable to take all the hemebilirubin formed, increasing hembilirubin concentration in the blood.