Download
1 / 55
550 likes | 713 Views
Pharmacologic in the Geriatric Population. Do you have a Pharm Dictionary?. www.nlm.nih.gov/medlineplus/mplusdictionary.html. Issues for the Geriatric Population. Pattern of drug use Altered response to drug therapy Multiple disease states Lack of proper drug testing

E N D
Do you have a Pharm Dictionary? • www.nlm.nih.gov/medlineplus/mplusdictionary.html
Issues for the Geriatric Population • Pattern of drug use • Altered response to drug therapy • Multiple disease states • Lack of proper drug testing • Problems with drug education and compliance (Health Literacy) • Financial issues impacting medication usage
Other Factors in Geriatric Drug Use • Presence of Multiple Chronic Conditions • 80% of those 65+ have multiple diseases with medications
Commonly prescribed meds related to ED admissions among elderly • From 2007 to 2009, 99,628 “emergency” hospitalizations of patients > 65 years of age occurred due to adverse drug events • 66% being attributed to unintentional drug overdose • 48% of the hospitalizations involving those > 80 years of age • 4 drugs were implicated in 67% of patients • Warfarin (33.3%) • Insulin (13.9%) • Anti-platelet agents (13.3%) • Oral hypoglycemic agents (10.7%)
Drug Interactions • Medscape Drug Interaction Checker www.medscape.com
Altered Response to Drugs • Pharmacokinetic Changes in the Body (The way in which one drug moves throughout the body) • Absorption • Metabolism • Distribution • Excretion
Pharmacokinetic change • Absorption • Altered GI function in elderly due to • Decrease gastric acid • Decrease stomach emptying • Decrease absorption area • Decrease motility • Sometimes decreased H2O intake
Pharmacokinetic change • Metabolism • The process to inactivate drugs and create water-soluble by-products (metabolites) that can be excreted by the kidneys. • Primarily takes place at liver • Interference with metabolism • MAO inhibitors (e.g. Selegiline) have lots of contraindications and drug interactions • Vitamin K with Coumadin • Vitamin B with Levodopa
Pharmacokinetic change • Hepatic Metabolism • Decrease liver mass • Decrease liver blood flow • Decrease enzyme activity Leads to decreased liver metabolism • Injury to liver (trauma, CA, ETOH also impact the liver metabolism)
Pharmacokinetic change • Distribution • Decrease in body water content • Increase in body fat • Decrease in lean body mass • Decrease in plasma proteins • e.g. aspirin or warfarin may produce a greater response because there will be less drug bound to • Drugs are area specific - either bind to receptors or act on tissues in order to be effective, e.g. water-soluble, fat soluble, protein affinity
Pharmacokinetic change • Excretion • Primarily takes place at kidney • Kidney filters the drug from the circulation and excrete it from the body via the urine • Decreased Renal functioning with age • Decrease kidney mass • Decrease renal blood flow • Decrease in tubular function in the nephron • Results in? Build up/Accumulation of drug
PharmacodynamicInteractions • The way in which one drug’s action interferes with the action of the other • Pharmacologic antagonism • Physiologic antagonism • Synergism
Pharmacodynamic Changes • Systemic drug response altered due to physiological changes in the elderly • Each patient is different in his response to medications • Altered response may occur with alterations in drug-receptor attraction which can increase or decrease sensitivity
Pharmacodynamic Changes • There are changes in receptor linkage or coupling to the cell that occurs in certain tissues as a function of aging. • In some patients the biological response of a medication may be blunted due to changes in cellular structure and function that occur in the elderly. • ½ life longer with aging adult
OTC drug use in Geriatrics • >60 y.o. 40% use OTC every day • Used for pain (OA), digestive purposes (laxative), decongestants (sometimes alcohol based) • 80% take with alcohol, Rx drugs or both • Use of alternative meds and treatment • can alter PT/PTT times, absorption
Psychotropic Drugs • Sedative Hypnotic? • Antianxiety Agents? • Antidepressant Meds? • Antipsychotic Meds • Haloperidol (Haldol)
Sedative Hypnotics • Benzodiazepine • Primary drugs used to promote sleep and decrease anxiety in older adults • Increase central inhibitory effect of GABA • Temazepam (Restoril) • Side effects • “hangover”, drowsiness and sluggish, anterograde amnesia (short-term memory for the period immediately preceding drug administration, rebound insomnia
Anti-Anxiety Meds • Decrease agitation • Drugs directly stimulating serotonin receptors in certain parts of the brain (dorsal raphe nucleus) • Benzodiazepine • Diazepam (Valium) • Lorezepam (Ativan) • Azapirones • Buspirone (BuSpar)=“Busy” drug decreases to help anxiety
Antidepressant • Increase synaptic transmission in CNS pathways that utilize norepinephrine, dopamine, or serotonin=same pathway • Tricyclic • Amitriptyline (Elavil)=“elevate your mood” • Produce anticholinergic (Ach) effects • dry mouth, constipation, urinary retention, and CNS symptoms such as confusion, cognitive impairment, and delirium. (frontal lobe)
Antidepressant • MAO inhibitors • Isocarboxazid (Marplan) • Causes orthostatic hypotension, insomnia. • 2nd generation (SSRI) • Bupropion (Wellbutrin) • Fluoxetine (Prozac) • Causes GI irritation and bleeding • May take anywhere from 1 to 6 weeks to take effect
Sinemet (Carbidopa/Levodopa) • Effective for mild to moderate Parkinson’s • Not effective for end stage. • GI problems • Nausea, vomiting • Cardiovascular problems • Arrythmia, orthostasis • Neuropsychiatric problems • Confusion, depression, anxiety, hallucination • On and OFF phenomenon • End of dose akinesia
FDA Warning about Stalevo(Carbidopa + Levodopa + Entacapone) • [Posted 08/20/2010] Issue: FDA notified healthcare professionals that it is evaluating clinical trial data that suggest patients taking Stalevo(a combination of carbidopa/levodopa and entacapone) may be at an increased risk for cardiovascular events (heart attack, stroke, and cardiovascular death) compared to those taking carbidopa/levodopa (sold as the combination product, Sinemet). http://www.nlm.nih.gov/medlineplus/druginfo/meds/a601068.html
Sinemet (Carbidopa/Levodopa) formulation • Coordinate patient care time at the peak effects of drug
Sinemet (Carbidopa/Levodopa) • The peak concentrations of levodopa after a single dose of Sinemet CR 50/200 increased by 25% when administered with food. • Vitamin B 6 can reduce the effects of levodopa when levodopa is taken by itself. • Large amounts of Vitamin B 6 are also contained in some foods, such as bananas, egg yolks, lima beans, meats, peanuts, and whole grain cereals. Patient should limit the amount of these goods while on Sinemet.
Pain and inflammation medications • Opiod Analgesics (aka Narcotics) • Morphine, Demoral, Codeine • Changes the pain perception but not painful stimulus • ADR: sedation, mood changes, nausea, vomiting, constipation, orthostatic hypotension, respiratory depression, drug addiction
Administration of morphine in the periaqueductal gray and serotonin (5-HT) in the Raphe nucleus produces analgesia. Fig 8.3B. neuroscience.uth.tmc.edu/s2/chapter08. html
Pain and inflammation medications • NSAIDs • Anagelsic, decrease inflammation and fever, anticoagulant • ADR: GI bleeding, renal and liver problems, impair bone healing • Acetaminophen • Analgesic, decrease fever • ADR: more toxic to liver than NSAIDs • NSAIDS and Acetaminophen inhibit the synthesis of prostaglandins at different sites.
Peripheral sensitization after an injury Fig 5.2 Harrison's Neurology in Clinical Medicine, 2010
Pain and inflammation medications • COX-2 inhibitor (Celebrex) • Inhibit the production of harmful prostaglandins • ADR: GI problems, cardiovascular problems such as MI and stroke (therefore VIOXX was removed from the market)
Pain and inflammation medications • Glucocorticoids • Anti-inflammatory (suppressing leukocyte and inhibit proinflammatory substances such as cytokines and prostaglandins) • ADR: HTN, peptic ulcer, aggravating DM, glaucoma, increased risk of infection, inhibit corticosteroids production by adrenal cortex • Glucocorticoids produce a general catabolic=destroyer effect throughout the body, breaking down bones, ligaments, tendons, skin and muscles
Cardiac Meds • Table 4-5
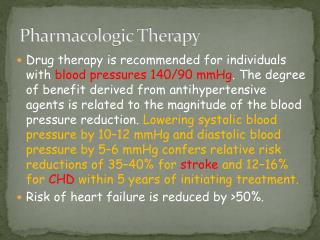
Drugs in geriatric hypertension • Current normal BP thresholds • Systolic/Diastolic BP < 140/90 mmHg in older adults • Systolic/Diastolic BP < 130/80 mmHg in older adults with comorbidities, e.g chronic renal insufficiency or diabetes mellitus • Hypertension T(x) Meds: B-blockers, Diuretics,
β-blockers, α-blockers (sympatholytic agents) • Reduce excessive sympathetic stimulation of the heart and peripheral vessels to decrease HR and myocardial contraction force • blocking epinephrine & norepinepherine • Indications of β-blockers: • HTN: Atenolol (Tenormin) • Angina: Metoprolol(Lopressor) • Arrthmias: Nadolol (Corgard) • CHF • β-blockers cause hypotension, dizziness, syncope
Diuretics • Indications: CHF, Hypertension, edema • Loop diuretic: Furosemide (Lasix) • Thiazide diuretic: Chlorothiazide (Diruil) • Potassium sparing diuretic: Spironolactone (Aldactone) • ADR: confusion, weakness, fatigue, increase urinary output (annoying side effects) • Common drug regimen • Diuretics + β-blocker • Diuretics + ACE inhibitor
Angina pectoris (chest pain – a symptom of coronary artery disease)
Organic Nitrates • Indications of organic nitrates • Angina pectoris: Nitroglycerin (nitrostat) • Sublingual or transdermal by a patch • ADR: decreased BP, orthostatic hypotension, dizziness
ACE Inhibitors (angiotensin-converting enzyme) • Block the conversion of Angiotensin 1 to Angiotensin 2 (a vasoconstrictor) and thus decrease the pressure in peripheral vasculature the heart pump against • Indications • HTN: Captopril (Capoten) • CHF: Enalapril (Vasotec) • ADR: hypotension, orthostatic hypotension • Common drug regimen • ACE inhibitor + Calcium blocker
Anti-Arrhythmic Medications • Sodium Channel Blockers • Lidocaine (Xylocaine) • Stabilize opening/closing membrane Na2+ channels to control myocardial excitability • β-Blockers • Nadolol (Corgard) • Prolong the duration of cardiac repolarization • Calcium Channel Blockers • Diltiazem(Cardizem) • Decrease myocardial excitability by limiting entry of Ca2+ into cardiac muscles
Pattern of Drug Use in the Elderly • Polypharmacy • Drug regime of a patient contains one or more “unnecessary” medications (both OTC and Rx meds) • Administration of drugs to treat an illness creates an adverse reaction, drug side effects seen as new symptoms. Therefore, more drugs are administered.
Characteristics of Polypharmacy • Use medication for no apparent reason • Use of duplicate medications • Use of concurrent interacting medications • Use of contraindicated medications • Use of inappropriate drugs • Use of drug therapy to treat adverse drug reactions • Patient improves when meds are discontinued
Prevention of Polypharmacy • Drug regime reviewed periodically • Written list, One pharmacy, Primary Care Physician • Unnecessary or harmful drugs are discontinued • Have family member discard expired drugs • New drugs added only if truly needed
Prevention of Polypharmacy • Communication between various physicians • PT’s can assist by recognizing changes in patient’s response to drugs • Identify changes as drug reactions rather than new symptoms • Have patient bring a list to therapy • Chart review
Common Adverse Drug Reactions (ADR) • GI problems • must adjust dose and type of medication to minimize problems • Sedation • many drugs will increase sedative properties in the elderly • Confusion • may increase in patients already confused
Other adverse drug reactions • Depression • Orthostatic Hypotension • Fatigue and Weakness • Dizziness and Falls • Extrapyramidal symptoms (dyskinesia) • Anticholinergic Effects • CNS effects with confusion, nervousness, drowsiness, dizziness • Dry mouth, constipation, urinary retention, tachycardia, blurred vision
Lack of Proper Drug Testing in the Geriatric Population • Evaluation of drugs in geriatric patients may not have occurred prior to FDA approval • In 1997, FDA established the Geriatric Use Subsection to provide guidance for labeling • Healthy People 2010: polypharmacy as a part of the safety issues (2020 as well)