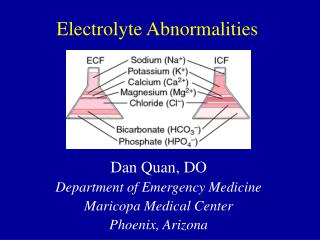
Electrolyte Abnormalities
Electrolyte Abnormalities. Oguchi Andrew Nwosu, MD, FAAFP Asst. Professor Emory Family Medicine July 26 th 2012. Goals. Review of common electrolyte abnormalities Normal ranges Clinical manifestations of hypo- or hyper- states Causes Treatment options. Goals.

Electrolyte Abnormalities
E N D
Presentation Transcript
Electrolyte Abnormalities Oguchi Andrew Nwosu, MD, FAAFP Asst. Professor Emory Family Medicine July 26th 2012
Goals • Review of common electrolyte abnormalities • Normal ranges • Clinical manifestations of hypo- or hyper- states • Causes • Treatment options
Goals • What will spend time on today… • Sodium • Potassium • Calcium • Magnesium • Phosphorus
Hyponatremia • Sodium: Normal 135 – 145 mg / dl • Symptoms usually begin <120 mg /dl • Nausea • Lethargy • Muscle cramps • Psychosis • Seizure • Coma • Death
Hyponatremia • Diagnosis based on assessment of serum osmolality and volume status
Hyponatremia • Serum Osmolality • Osmolality (calculated) = 2 (Na) + Gluc / 18 + BUN /2.8
Hyponatremia • Normal Osmolality (280 – 295 mOsm / kg) Isotonic pseudohyponatremia Hyperproteinemia (>10 mg / dl) Hyperlipidemia (severe)
Hyponatremia • High Osmolality (>300 mosm / kg) Hypertonic hyponatremia Hyperglycemia Na: 1.6 mEq / liter decrease per 100 mg/dl increase in glucose Mannitol excess Glycerol therapy Am J Med 1999 Apr;106(4):399-403
Hyponatremia • Low serum osmolality (<280 mOsm / kg) Hypotonic hyponatremia Need to assess volume status next in these patients.
Hypotonic hyponatremia • Hypovolemia • GI losses • Renal losses plus excess water ingestion • Third space losses Tx: Isotonic saline
Hypotonic Hyponatremia • Hypervolemia • CHF • Liver disease • Nephrotic syndrome • CKD Urine Na: < 20 mEq /liter except in CKD Tx: Salt restriction / water restriction / diuretics
Hypotonic Hyponatremia • Isovolemia • Glucocorticoid insufficiency • Hypothyroidism • Psychogenic polydipsia • Medications (amitriptyline / cyclophosphamide / carbamazepine / morphine) • SIADH • Diuretic use with potassium depletion
Isovolemic Hypotonic Hyponatremia • SIADH • Syndrome of inappropriate antidiuretic hormone • Hypotonic hyponatremia • Clinical euvolemia • Inappropriately elevated urine osmolality in face of low serum osmolality • Urine Na >20 mEq / liter • Normal renal function / TSH / cortisol
SIADH • Acute tx • Severe hyponatremia (<110 mEq / liter) • IV lasix • NS with 20 – 40 mEq / liter KCL • Rarely 3% saline will be needed • Chronic tx • Mild hyponatremia • Water restriction to approx 1000 ml / day • Demeclocycline 300 mg PO bid if water restriction not working (contraindicated in liver disease)
SIADH • Chronic treatment (cont) • Vasopressin receptor antagonists • Conivaptan (Vaprisol) IV prep
Hyponatremia • Treatment principles • Not too fast (pontine myelinolysis) • Symptomatic • Initial 1 - 2 mEq / L / hr x two hours, then • 0.5 mEq / L / hr • Asymptomatic • 0.5 mEq / L / hr • Max in 24 hours: 10 meq total rise • Max in 48 hours: 18 meq total rise Am J Med. 2007 Nov;120(11 Suppl 1):S1-21.
Hypernatremia • Sodium: Normal 135 – 145 mg / dl • Clinical manifestations • Tremors • Irritability • Ataxia • Spasticity • Mental confusion • Seizures • Coma • Death
Hypernatremia • Cause: • Net sodium gain • Net water loss
Hypernatremia • Volume expansion (net sodium gain) • Cause • Hypertonic saline / NaHCO3 administration • Primary hyperaldosteronism • Cushing’s syndrome Tx: Diuretics D5W to replace fluid loss after diuretics
Hypernatremia • Water depletion • Hypotonic fluid losses
Hypovolemic hypernatremia • Treatment • Calculate free water deficit
Hypovolemic hypernatremia • If hemodynamic compromise, then replace initially with NS • Otherwise use ½ NS or D5W • Aim to decrease Na by 0.5 mEq / liter / hr • Correct one half of the water deficit in 24 hrs • Correct other half over next 24-48 hours
Hypovolemic hypernatremia • Diabetes insipidus Sxs: Polyuria / Polydipsia / Low urine osm • Central • Tumor / Granuloma / Trauma / Surgery • Nephrogenic • Severe hypokalemia / hypercalcemia / CKD / Drugs (lithium / demeclocycline / amphotericin)
Hypovolemic hypernatremia • DI • Differentiation of central and nephrogenic • Trial of water deprivation • Failure to concentrate urine confirms DI • Subsequently given arginine vasopressin • Central DI (urine concentration increases) • Nephrogenic DI (no increase)
Hypovolemic hypernatremia • DI • Treatment • Central • DDAVPP 5-10 mcg intranasally q day / bid • Nephrogenic • Correction of underlying cause if possible • Genetic abnl / lithium / hypercalcemia • Thiazide diuretic / salt restriction can help
Hypokalemia • Normal K level: 3.5 – 5.0 • Clinical manifestations • Fatigue • Cramps • Constipation • Weakness / Paralysis • Paraesthesias • Arrhythmias
Hypokalemia • EKG abnormalites • Flattened T waves • ST depressions • Prominent U waves http://www.merck.com/media/mmpe/figures/MMPE_12END_156_02_eps.gif
Hypokalemia • Causes • Inadequate intake • GI losses • Renal losses • Acid-base shifts • Hypomagnesemia • Hyperaldosteronism • Medications (diuretics)
Hypokalemia Treatment • Oral therapy • Mild hypokalemia • Increase dietary intake • Potatoes / Bananas • KCl preps (i.e. KDur) • Preps can be used in range 8 – 20 mEq • Monitor K level and adjust dose as needed • Correct cause
Hypokalemia Treatment • IV repletion • Severe hypokalemia • Inability to tolerate oral repletion Max Concentration: 60 mEq / liter Note pain is common at > 40 mEq /liter Rate: 10 mEq / hr (20 mEq / hr with tele) Monitor response and decrease conc / rate as appropriate.
Hyperkalemia • Potassium Normal 3.5 – 5.0 • Elevated potassium level should be evaluated as to the following: • What is the cause? • Is the cause an acute or chronic issue? • Are there accompanying EKG changes?
Hyperkalemia • Symptoms • Usually asymptomatic • Muscle weakness / paralysis • EKG abnormalities • Peaked T waves • ST depression • 1st degree AVB/Loss of P wave • QRS widening • “Sine wave sign”
Hyperkalemia • EKG changes
Hyperkalemia • Think about the cause • 1. Too much total potassium • Renal disease • Intake increased (rare outside of renal disease) • 2. Shift of potassium from intracellular space to extracellular space • DKA
Hyperkalemia • Does the potassium level make sense in the patient? Pseudohyperkalemia (hemolysis)
Hyperkalemia • When do we treat • Patient assessment • Cause • Chronicity • Degree of potassium elevation • <6.0 Does not need acute invasive tx • >6.0- 6.5 Kayexalate +/- other modalities • >6.5 Consider more acute modalities
Hyperkalemia • Treatment options • Calcium gluconate • NaHCO3 • Regular insulin • Albuterol nebulizer treatment • Kayexalate • Dialysis
Hyperkalemia • Calcium gluconate • IV formulation is 1000 mg / 10 ml (10% soln) • Dose: 10 ml over 2-5 minutes IV with EKG monitoring • Action: Stabilization of cardiac cells. Does not lower K. Used for hyperkalemia with EKG changes. • If EKG changes do not immediately resolve, repeat in 5 minutes. • Will worsen Dig Toxicity
Hyperkalemia • Beta agonist • Albuterol nebulizer treatment • 2-4 ml of 0.5% soln (10-20 mg dose) • Epinephrine IV infusion • Insulin • Regular insulin 10 units IV plus one D50 Amp over 5 minutes. • Follow this with a D 5 containing IV maintenance fluid for several hours.
Hyperkalemia • Kayexalate (Na – K exchange resin) • PO dosing: 15 -30 gram • Can be mixed with 60-120 ml of a 20% sorbitol soln to avoid constipation • PR dosing: 50 grams • Mix with 50 ml of 70% sorbitol and 100 ml tap H20 • Retain in rectum x 30 minutes minimum but ideally 2+ hours
Hypocalcemia • Normal Calcium: 8.9 – 10.3 mg/dl • Calcium • 40% bound to albumin • 15% bound to other serum anions • 45% is ionized in serum
Hypocalcemia • Correct for low albumin • 0.8 mg / dl drop in Calcium for every 1 g / dl drop in Albumin • Corr Ca = Meas Ca + (0.8 * (4.5 – Meas Alb))
Hypocalcemia • Clinical signs of low calcium: • Tetany / Carpopedal spasm • Trousseau’s sign • Chvostek’s sign • Lethargy / confusion • Seizures • Heart failure • EKG: Prolonged QT
Hypocalcemia • Treatment of symptomatic cases • Calcium gluconate (10% soln) which contains 100 mg elem calcium / 10 ml. 1. Give two ampules IV over 10 minutes then 2. Add six ampules to 500 ml D5W and infuse at 1 mg / kg / hr
Hypocalcemia • Asymptomatic • Calcium orally (1000 mg / day) • Vit D orally • Calcitriol 0.25 – 0.5 mcg / day
Hypocalcemia • Magnesium can be effective as well • Magnesium sulfate 2 gram IV bolus followed by 1 gram / hr gtt
Hypercalcemia • Calcium range: 8.9 – 10.3 mg / dl • Symptoms • Anorexia • N/V • Constipation • Polyuria • Nephrolithiasis • Weakness • Confusion • Coma • EKG: Shortened QT interval
Hypercalcemia : Causes • Primary hyperparathyroidism • Malignancy • Sarcoidosis • Vitamin D toxicity • Hyperthyroidism • Thiazide diuretics • Milk-alkali syndrome • Renal failure • Familial hypocalciuric hypercalcemia • Immobilization