Download
1 / 51
520 likes | 562 Views
The Digestive System M 230A students Dr. Mukhallad Al-Janabi د. مخلد عبدالمنعم الجنابي. The digestive system consists of a tract plus the accessory organs.

E N D
The Digestive SystemM 230A studentsDr. Mukhallad Al-Janabiد. مخلد عبدالمنعم الجنابي
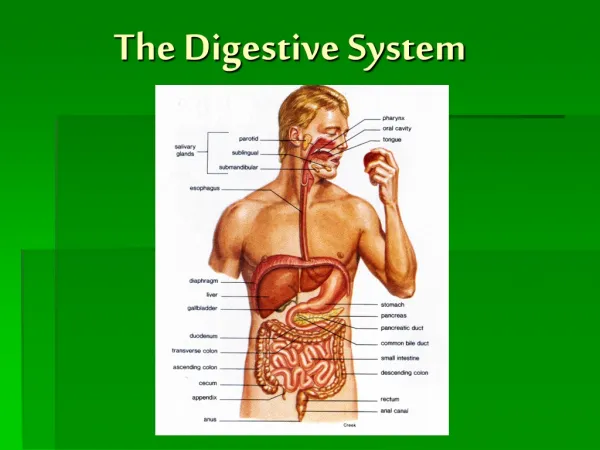
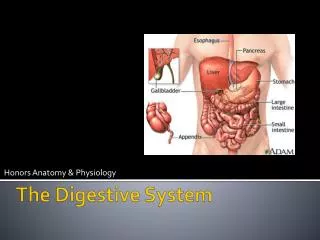
The digestive system consists of a tract plus the accessory organs. • The tract is a continuous tube that consists of the mouth, pharynx, esophagus, stomach, small intestine, large intestine, and anus. Ingested contents pass through these organs in this order. • The accessory organs are the salivary glands, pancreas, and biliary system (liver and gallbladder).
Four main processes (functions)occur in digestive system • This system has four functions: 1.Motility is the muscular contractions that mix (mixing movements) and move (propulsive movements) the contents forward through the digestive tract. 2. Secretion is the transfer of digestive juices by exocrine glands into the digestive tract. The digestive secretion consists of water, electrolytes and organic substances like enzymes, bile salts and mucus. The secretions are controlled by neural or hormonal factors.
Functions of digestive system (continued) • 3. Digestion is break down of food into smaller unites which can be absorbed. It involves chemical change (hydrolysis) of large molecules by digestive enzymes (e.g., carbohydrates, proteins, and fats) into their smaller subunits (e.g., starch into glucose, proteins into amino acids, etc). An example of hydrolysis: the disaccharide maltose (the intermediate breakdown product of polysaccharides) is broken down into two glucose molecules by the addition of H2O at the bond site. Glucose Glucose Maltose • 4. Absorption is the passage of the products of digestion (e.g., monosaccharides like glucose, amino acids and fatty acids), along with water, vitamins, and electrolytes, into the blood and lymph.
Extra points about digestive processes • The smooth muscle in the walls of the digestive tract maintains a low level of contraction called tone. There are two types of digestive motility: propulsive movements and mixing movements. Propulsive movements push the contents forward through the tract. Mixing movements help in digestion and absorption. • Digestive secretions consist of water, electrolytes, and organic constituents such as enzymes, bile, salts, and mucus. They are released by hormonal or neural stimulation. • Polysaccharides (e.g., starch and glycogen) are chemically changed into disaccharides, which are changed into monosaccharides. Proteins are chemically changed into polypeptides, which are changed into amino acids. The end products of fat digestion are monoglycerides and free fatty acids. • Most absorption occurs in the small intestine.
Digestive motility and secretion are regulated by four factors. • Smooth muscle cells display rhythmic, spontaneous variations in membrane potentials. This is autonomous smooth muscle function. • The myenteric plexus and submucous plexus are the enteric nervous system (collection of neurons within the wall of GIT tract). • Extrinsic nerves of the autonomic nervous system innervate digestive structures from the outside. They modify digestive tract motility and secretion. Parasympathetic nerves signal maximum digestive activity. • Endocrine glands within the mucosa release hormones that signal digestive responses. • Within GIT there are chemoreceptors, mechanoreceptors, and osmoreceptors respond to changes in the digestive tract.
External influence Local changes in digestive tract Receptors in digestive tract Extrinsic automatic nerves Intrinsic nerve plexuses Gastrointestinal hormones Smooth muscle (contraction for motility) Exocrine gland cells (secretion of digestive juices) Endocrine gland cells (secretion of gastrointestinal and pancreatic hormones) Self- excitable = Short reflex = Long reflex = Hormonal pathway
The wall of the digestive tract consists of four layers. 1. The mucosa lines the luminal surface. The lamina propria is a middle layer of connective tissue. The muscularis mucosa is a sparse layer of smooth muscle. 2. The submucosa is under the mucosa This connective tissue has large blood and lymph vessels. It contains a submucous plexus. 3. The muscularis externa is the main smooth layer of the digestive tube. It has an inner circular layer and an outer longitudinal layer. Their contractions produce the propulsive and mixing movements. A myenteric plexus is between the two smooth muscle layers. 4. The serosa is the outer connective tissue layer. It is continuous with the mesentery along much of the tract.
The oral cavity is the entrance to the digestive tract. • Salivary secretion is continuous and can be reflexly increased. Salivary Flow: 1-2 L/day • Basal rate is about 0.5ml/minute • Maximum secretion 5 ml/minute The amylase enzyme in salivary secretion digests starch into maltose. Lysozyme in the saliva lyses bacteria. • Saliva also keeps the mouth and teeth clean. • Both branches of the autonomic nervous system increase the rate of stimulation.
Function of Saliva 1. Moistens oral mucosa. It facilitates speaking , chewing and swallowing. 2. Moistens dry food, lubricates food to facilitate swallowing and cools hot food. 3.Provides a medium for dissolved foods to stimulate the taste buds. 4. Buffers oral cavity contents. Saliva has a high concentration of bicarbonate ions. It neutralizes acid in the food 5. Digestion. Amylase, contained in saliva, breaks polysaccharides into maltose. 6. Neutralizes any gastric acid that refluxes from stomach into the lower esophagus. 7. Controls bacterial flora of the oral cavity by: • Presence of enzyme called Lysozyme: lyses (destroys) certain bacteria by breaking their wall • Washing (rinsing) away remained food which acts as a food source for bacteria ** Absence of salivary secretion (xerostomia) leads to • Difficulties in swallowing, talking and chewing • Dental caries.
Saliva production is controlled by salivary center in medulla through autonomic nervous system. Salivary secretion is the only digestive secretion that controlled only by neural factors *Excitation of parasympathetic nerve fibers causes: Increased watery secretion rich in electrolytes and enzymes. *Excitation of sympathetic nerve fibers causes: -slight increase in viscid saliva (containing mucus). Innervation of salivary glands
Swallowing Swallowing center inhabits respiratory center in brain stem Oropharyngeal stage: **moving the bolus from mouth through pharynx and then into esophagus. **The following events occur during this stage a. Uvula is elevated to prevent food to enter into nasal cavity. b. Food is prevented from entering into trachea (respiratory system) by the following events • Elevation of larynx • Closure of glottis by closure approximation of vocal cords • Epiglottis tilted backward to cover the larynx • Respiration is stopped Elevation of uvula prevents food from entering nasal passages Epiglottis is pressed down over closed glottis as auxiliary mechanism to prevent food from entering airways Tight apposition of vocal folds across glottis prevents food from entering respiratory airways
Swallowing (continued) • Involuntary swallowing is initiated when a food bolus contacts receptors in the pharynx. Afferent impulses are sent to the swallowing center in the medulla. This triggers various swallowing responses. • The pharyngoesophageal sphincter prevents air from entering the digestive tract during breathing. The sphincter keeps the esophagus closed. • Peristalsis waves push food through the esophagus. • A swallowing center initiates a primary peristaltic wave. • The gastroesophageal sphincter prevents reflux of gastric contents. • Esophagus secretes only mucus which protects the esophygeal lining against sharp edges of food and against any acid and enzyme of gastric juice if gastric reflux occurs. Ringlike peristaltic contractions push bolus down
The stomach • Stomach has a fundus, body, and antrum. Its terminal part has a pyloric sphincter. ****One function of the stomach is to store food. Most of this occurs in the body of the stomach. • The stomach accommodates a twenty-fold increase in volume by receptive relaxation. • It also secretes HCl and pepsinogen enzyme to begin protein digestion. ****The mixing movements of the stomach mix food with gastric juice producing chyme. • Most of this mixing occurs in the antrum.
Gastric movements **Mixing movements Occur mostly in antrum They mix the food with gastric content to produce chyme They are peristaltic contractions against closed pyloric sphincter **Propulsive movements The peristaltic movements themselves push the chyme through pyloric region where chyme can leave stomach to duodenum Pyloric sphincter Peristaltic contraction
Gastric emptying • After food is digested and mixed by peristalsis with gastric juice in the stomach. It is converted into chyme which is pushed by gastric motility into the small intestine. ***Gatric motility is increased by 1. Distension of the stomach 2. Signaling by the vagus nerve 3. the hormone gastrin ***Duodenal factors that decreases the gastric emptying. a. Presence of undigested fat b. Presence of acid c. an increase in osmolarity of the chyme d. Distension of the duodenum. ***Gastric emptying is inhibited by the following hormones a. Secretin b. CCK
Stomach Esophagus Gastroesophageal sphincter Pyloric sphincter Duodenum Direction of movement of peristaltic contraction Peristaltic contraction Movement of chyme Gastric emptying Fig. 15-8a, p. 477
VOMITING ***It is forceful expulsion of gastric contents out through the mouth. • The stomach does not activelyparticipate in vomiting. The stomach, esophagus and upper and lower esophageal sphincters are relaxed • The force of vomiting arises from contraction of the diaphragm and abdominal muscles. These contractions leads to increased intra-abdominal pressure. The stomach is relaxed and squeezed to evacuate the food during vomiting. It is coordinated by the vomiting center in the medulla. During vomiting glottis is closed to prevent passage of vomited materials into respiratory passages. Respiration is also inhibited during vomiting. ****Causes of vomiting include tactile stimulation, irritation/distension of the stomach and duodenum, elevated intracranial pressure, chemical agents, and psychogenic factors. ***Severe vomiting can lead to dehydration, metabolic alkalosis and circulatory problems.
Gastric digestive juice ***Mucous cells secrete mucus. ***Parietal cells secrete HCl and the intrinsic factor. This factor is essential for the absorption of vitamin B12. The exocrine secretions of these cells are released into the gastric lumen. • Other secretory cells of the gastric mucosa release endocrine and paracrine regulatory factors. • The low pH in the stomach converts pepsinogen into the active form, pepsin. • Functions of hydrochloric acid in the stomach include pepsin formation, the breakdown of connective tissue and muscle fibers, the denaturation of proteins, and the killing of most microorganisms. • A mucus lining on the surface of the gastric mucosa is protective against acidity.
Parietal and chief cells • Acetylcholine from the intrinsic nerve plexuses stimulates these cells. • Histamine acts on parietal cells to increase hydrochloric acid secretion. • Gastrin (secreted by G cells) stimulates parietal and chief cells. • Somatostatin (secreted by D cells) inhibits secretions from parietal cells. • The control of gastric secretion involves three phases. 1. Cephalic phase: stimuli from the brain like thinking, tasting, smelling and chewing increase the secretion of hydrochloric acid and pepsinogen. 2. Gastric phase: stimuli in the stomach (e.g., proteins) distension initiate gastric secretions. 3. Intestinal phase: it is inhibitory, decreasing secretion of gastric juices.
Other facts about stomach activity include: • The stomach lining is protected from gastric secretions by the gastric mucosal barrier. The mucosal membrane is almost impermeable to hydrogen ions. • Carbohydrate digestion continues in the body of the stomach. Proteins digestion begins in the antrum. Salivary amylase continues to work in the internal mass of food. Food is not mixed with gastric secretions in the body of the stomach. • The stomach absorbs alcohol and aspirin, but does not absorb food.
Gastric secretion is decreased by many factors: 1. Accumulation of acid in the stomach 2. As food leave the stomach, the protein concentration in the stomach is decreased and there is less distension of the stomach 3. When food reaches duodenum: presence of fat, acid, hypertonicity and distension of duodenum sends inhibitory signals to gastric mucosa to decrease the secretion
The pancreas has exocrine and endocrine cells • Endocrine cells of the islets of Langerhans secrete hormones. • The exocrine pancreas secretes digestive enzymes and an aqueous alkaline fluid. The alkaline fluid has sodium carbonate. • The enzymes are proteolytic enzymes, pancreatic amylase, and pancreatic lipase. 1. Trypsin, formed from trypsinogen, is a proteolytic enzyme. Chymotrypsinogen and procarboxypeptidase are other proteolytic enzymes. 2. Pancreatic amylase converts starch to disaccharides. 3. Pancreatic lipase hydrolyzes dietary lipids. • Pancreatic exocrine secretion is regulated by secretin and cholycycstokinin (CCK), enzymes secreted by the small intestine. **Secretin causes secretion of sodium bicarbonate from the pancreas. **CCK regulates the secretion of pancreas digestive enzymes.
Bile duct from liver Duodenum Stomach Hormones (insulin, glucagon) Blood Endocrine portion of pancreas (Islets of Langerhans) Duct cells secrete aqueous NaHCO3 solution Acinar cells secrete digestive enzymes The glandular portions of the pancreas are grossly exaggerated Exocrine portion of panaceas (Acinar and duct cells)
Fat and protein products in duodenal lumen Acid in duodenal lumen Secretion release from duodenal mucosa CCK release from duodenal mucosa (Secretin carried by blood) Neutralizes (CCK carried by blood) Digests Pancreatic acinar cells Pancreatic duct cells Secretion of pancreatic digestive enzymes into duodenal lumen Secretion of aqueous NaHCO3 solution into duodenal lumen
Pancreatic digestive enzymes • Pancreas secrets two types of secretion 1. Pancreatic enzymes from pancreatic acinar cells. containing: a. proteolytic enzymes (trypsinogen, chymotrypsin and procarboxypeptidase). All these enzymes are secreted in inactive forms. In duodenal lumen trypsinogen is activated by entrokinase enzyme converting it into trypsin. Trypsin activates chymotrypsin and procarboxypeptidase. b. Pancreatic amylase (secreted as active form) hydrolyzes starch into disaccharides c. Pancreatic lipase (secreted as active form) acts on fat producing fatty acids and monoglycerides 2. Watery alkaline secretion from the pancreatic ducts for neutralizing the acid chymeand providing alkaline environment for optimal activity of pancreatic digestive enzymes.
Liver functions • It carries out the metabolic processing of nutrients. • It detoxifies or degrades body wastes. • It synthesizes plasma proteins. • It stores substances such as glycogen and fats. • It activates vitamin D. • It removes bacteria and worn-out old RBCs. • It excretes cholesterol and bilirubin. Blood enters the liver from the digestive tract by the hepatic portal system. The portal vein of this system breaks into a capillary network, the liver sinusoids. The liver lobules are delineated by vascular and bile channels. Hepatocytes continuously secrete bile into these channels. Bile ducts from the lobules in the liver converge to form the common bile duct. This duct transports bile from the liver to the duodenum. Bile is stored in the gallbladder between meals. After a meal the gallbladder secretes bile into the small intestine for fat digestion. Hepatic artery Portal vein
Bile salts aid fat digestion and absorption • The detergent action of bile emulsifies fats. Fat globules are broken into smaller droplets, increasing surface area to facilitate enzymatic attack (pancreatic lipase). • Pancreatic lipase is attached to a fat droplet by the polypeptide colipase. • Bile salts adsorb on the surface of small fat droplets, preventing the droplets for recoalescing. This also helps enzymatic attack. • Bile salts are the most potent stimulus for increased bile secretion. Its secretion occurs by a chemical mechanism, hormonal mechanism, and a neural mechanism. • Bilirubin is a waste product excreted in the bile.
Negativity charged H2O-soluble portion (a carboxyl group at the end of a glycine or taurine chain) Small lipid (fat) droplet with bile salt molecules absorbed on its surface Lipid-soluble portion (derived from cholesterol)
Large fat droplet Through action of bile salts Lipid emulsion
Micelle structure: it has two components A. Outer is hydrophilic (water soluble) B. Inner is lipophilic (lipid soluble ) Hydrophobic core Hydrophilic shell Water-soluble portion Water-soluble portion lipid-soluble products of fat digestion like cholesterol, Fatty acids and monoglycerides Lipid-soluble portion Lipid-soluble portion Bile salt Lecithin
The small intestine is where most digestion and absorption occur. • Its three segments are the duodenum, jejunum, and ileum. • The process of segmentation mixes and slowly propels the food. • Segmentation mixes chyme with secretions and slowly moves the contents through the tract. • The circular smooth muscle responsiveness is influenced by the distension of the intestine, gastrin, and extrinsic nerve activity. • The ileocecal valve between the small and large intestine. It prevents contamination of the small intestine by colonic bacteria.
Other facts about the small intestine • It does not secrete digestive enzymes. The pancreas secretes enzymes into small intestine. • The small intestine enzymes complete digestion intracellularly (inside intestinal epithelial cells). These include the disaccharidases and aminopeptidases. • The mucosal lining has a rapid turnover. The crypts of Lieberkuhn have stem cells for cell regeneration.
The small intestine has adaptations to maximize absorption. The mucosal lining has a large surface area due to its circular folds and fingerlike projections called villi. The epithelial cells also have microvilli. All these factors will increase the surface area of absorption 600 times Circular fold Villus (Continue to next slide)
Epithelial cell A villus has a cover of epithelial cells, a capillary network, and the terminal lymphatic vessel. During absorption molecules produced by digestion enter the capillary or lymphatic vessel. Capillaries Mucous cell Central lacteal Crypt of Lieberkühn Arteriole Venule Lymphatic vessel Microvilli
Absorption of carbohydrates and proteins • Glucose and galactose are absorbed from intestinal lumen into the interior of intestinal cells by secondary active transport with Na+. They are cotransported with sodium. Glucose and galactose leave the intestinal cell into extracellular fluid by facilitated diffusion. • Fructose is absorbed by passive facilitated diffusion. • Amino and small peptides are absorbed across intestinal cells by secondary active transport with Na+.
Absorption of water • Energy-dependent sodium transport absorption drives passive water absorption. • Sodium is pumped from the tract lumen into the interstitial fluid. From there it enters capillaries by diffusion. • The transport of sodium creates an osmotic pressure. Water follow the sodium as it is absorbed.
Fat absorption • Monoglycerides and free fatty acids are produced by hydrolysis of lipids. • These water-insoluble products are carried to the inside of water-soluble micelles. • On the mucosal surface these molecules leave the micelle and passively diffuse through the lipid bilayer of the luminal membrane. They are resynthesized into triglycerides inside the epithelial cells. There they form water-soluble chylomicrons which leave the cells by exocytosis. • They enter the central lacteals, lymphatic vessels.
Lipid emulsion Micelles diffusion Lumen Lumen Micelle Micelles Microvillus Fatty acids, monoglycerides Aggregate and coated with lipoprotien Passive absorption Short or medium chain Basement membrane Epithelial cell of villus (Exocytosis) Capillary Central lacteal
Adsorption of vitamins, iron and calcium • Vitamin adsorption is mainly passive. Water-soluble vitamins are absorbed with water. Fat-soluble vitamins are absorbed in micelles. • Iron and calcium absorption is regulated. Only a part of ingested iron can be absorbed. • Some absorbed iron is immediately transported to the blood. Transferrin carries some iron to the bone marrow. Excess iron is stored in the ferritin pool. Unused iron is lost in the feces. • Most calcium is absorbed by active transport. About two-thirds of ingested calcium is absorbed. The remaining one-thirds is eliminated. • Most absorbed nutrients immediately pass through the liver for processing. The liver monitors nutrient molecules and controls their concentration in the blood or lymph leaving the liver.
Large intestine • It consists of the colon, cecum, appendix, and rectum. • The colon consists of the ascending colon, transverse colon, descending colon, and sigmoid colon. • Most digestion and absorption has been accomplished in the small intestine. The colon receives indigestible food, unabsorbed biliary components and the remaining fluid. • The colon absorbs water and salt and eliminates the feces.
Large intestine (continued) **Contractions of the haustrae slowly shuffle the colonic contents back and forth. They are initiated by the autonomous rhythmic contractions of the smooth muscle in the wall of the large intestine. • The large-intestine secretion is entirely protective. It consists of an alkaline mucus solution which protects the intestinal mucosa.
Large intestine (continued) ***The colon contains many beneficial bacteria. Their functions include • making vitamin K 2. Enhancing intestinal immunity 3. Increasing colonic motility • Mass movements propel colonic contents long distances. They occur three to four times a day and usually after meal. They drive the feces into the distal part of the large intestine and hence triggering defecation reflex.