THE COMPLEMENT SYSTEM
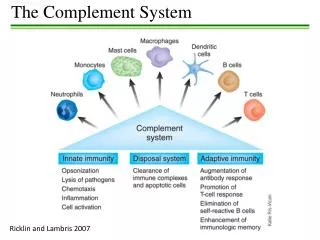
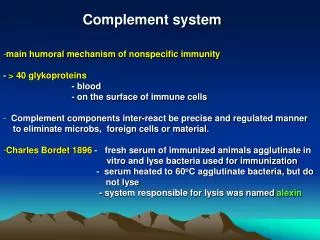
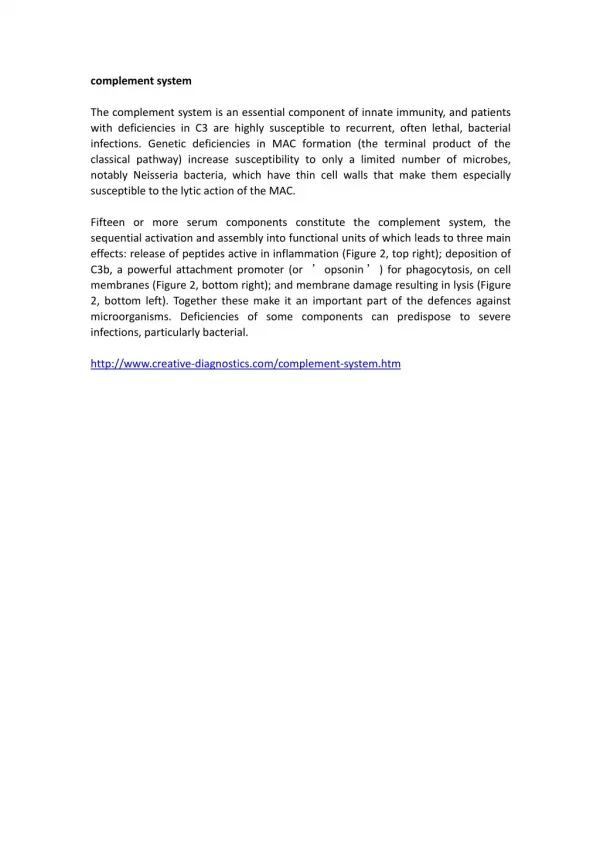
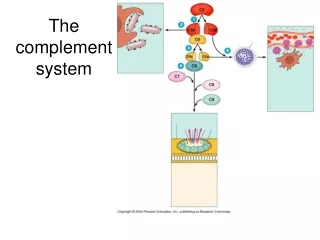
THE COMPLEMENT SYSTEM. Complement system. The complement system is a set of plasma proteins that act in a cascade to attack and kill extracellular pathogens. Approximately 30 components: - activating molecules - regulator factors - complement receptors

THE COMPLEMENT SYSTEM
E N D
Presentation Transcript
Complement system The complement system is a set of plasma proteins that act in a cascade to attack and kill extracellular pathogens. Approximately 30 components: - activating molecules - regulator factors - complement receptors - membrane proteins wich inhibit the lysis of host cells Most of the complement proteins and glycoproteins are produced in the liver in an inactive form (zymogen). Activation is induced by proteolitic cleavage.
AMPLIFICATION OF THE COMPLEMENT CASCADE limited proteolysis inactive precursors enzyme activating surface Activating surface needed!
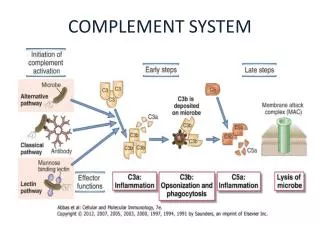
ACTIVATION OF THE COMPLEMENT SYSTEM COMPLEMENT ACTIVATION RECRUITMENT OF INFLAMMATORY CELLS OPSONIZATION OF PATHOGENS KILLING OF PATHOGENS
The classical pathway of complement activation is initiated by antibodies
Classical pathway THE C1 COMPLEX Collagen „legs” Gobular „heads” C1 is always present in serum but it can operate on an activating surface in normal case Low affinity binding to the C-terminal of antibody - Multiple interaction with immune complexes Only in classical pathway!
The classical pathway: Fixation of complement, generation of C3b by the classical C3 convertase Due to a double nomenclature present in terminology, the larger fragment of C2 can be indicated by C2a and C2b too. The classical C3 convertase is always composed of the larger fragments of C2 and C4 regardless of the name used!
THE CENTRAL COMPONENT OF THE COMPLEMENT SYSTEM Complementfixation (3900000000000000 molecules/ml)
Different isotypes of antibodies activate the complement system differently
Eukariotic cells Mannose GLYCOSYLATION OF PROTEINS IS DIFFERENT IN VARIOUS SPECIES Prokariotic cells Galactose Glucoseamine Neuraminic acid (sialic acid) Mannose
MANNAN-BINDING LEKTIN ACTIVATES THE COMPLEMENT SYSTEM MASP = MBL associated serin protease
Activation of the alternative pathway C3b from classical or the lectin pathway initiates the alternative pathway
Membrane attack complex (MAC) C3-convertase + C3b= C5 convertase
The membrane-attack complex assembles to generate a pore in the lipid bilayer membrane liveand dead bacteria MAC in the cell membrane
Classical pathway Lectin pathway Alternative pathway C1 (C1q + C1r,C1s) MBL (MASP-1,2) C3C3b (+C3a) D C3bBbC3b+B (+Ba) C4, C2C4b2b (+C4a, C2a) C4b2b+C3bC4b2b3b C3bBb3bC3bBb+C3b C5C5b (+C5a) C5b + C6 + C7 + C8 +10-16db C9 (polimerization) MAC C3 convertase complex(es) C3C3b(+C3a) C5 convertase complex(es)
Regulatory proteins on human cells protect them from complement-mediated attack
CD59 prevents assembly of terminal complement components into a membrane pore
Major regulating factors of complement system C1Inh: C1-inhibitor (serine-protease inhibitor) Factor I: inhibits both C3 convertases in the presence of co-factors (C4bp – classical pw., factor H – alternative pw., MCP – both) Properdin: ballasts convertases of alternative pathway DAF(CD55): Decay Accelerating Factor MCP: Membrane Cofactor Protein MIRL(CD59): Membrane Inhibitor of Reactive Lysis
Factor I DAF C1Inh C4bp CR1 MCP HRF C-pept.ase N CD59 S-protein DAF Fact-H CR1 MCP Factor I positive feedback Regulation of complement system a-2macrogl LECTIN PATHWAY Properdin membrane protein soluble molecule
C3b C3b C3b C3b C3b inflammation phagocytosis The role of complement system in in vivo Alternative, lectin & classical pathway C3 MAC lysis C3a C4a C5a opsonization
bacterium complement receptor macrophage OPSONIZATION C3b
Local inflammatory responses can be induced by the small complement fragments C3a, C4a, and especially C5a
Deficiencies of complement system – cascade molecules Not the lysis of cells is the most important function of the complement system
One of the major function of C1 INHIBITOR C1q binds to IgM on bacterial surface C1q binds to at least two IgG molecules on bacterial surface Binding of C1q to Ig activates C1r, which cleaves and activates the serine protease C1s C1INH dissociates C1r and C1s from the active C1 complex
Hereditary angioneurotic edema (HANE) (hereditary C1INH defect) • 17-year old boy - severe abdominal pain (frequent sharp spasms, vomiting) • appendectomia normal appendix • similar symptoms occured repeatedly earlier in his life with watery diarrhea • family history of prior illness • immunologist’s suspicion: hereditary angioneurotic edema • level of C1INH: 16% of the normal mean • daily doses of Winstrol (steroid) – marked diminution in the frequency and • severity of symptoms • intravenous purified C1INH became avaible by the time • Main symptoms: • swellings of skin, guts, respiratory tracts • serious acute abdominal pain, vomiting • larynx swelling – suffocation, may cause death • Treatment: • iv C1INH, FFP, steroid • kallikrein and bradykinin receptor antagonists Child with symptoms of HANE
Pathogenesis of hereditary angioneurotic edema Inhibition by C1INH in many steps activation of XII factor • bradykinin and C2-kinin: • enhance the permeability of • postcapillar venules • by contraction of endothel • holes in the venule walls • edema formation • C1 is always active without • activating surface because • plasmine is always active activation of kallikrein activation of proactivator cleveage of kininogen to generate bradykinin, vasoactive peptide cleveage of C2a to generate C2-kinin, vasoactive peptide cleveage of plasminogen to generate plasmin cleveage of C2 to generate C2a activation of C1
Questions hereditary angioneurotic edema 1. Activation of complement system results in the release of histamine and chemokines, which normally produce pain, heat and itching. Why is the edema fluid in HANE free of cellular components, and why does the swelling not itch? Histamine release on complement activation and recruiting of leukocytes is caused by C3a and C5a, both generated by the C3/C5 convertases. In HANE C1 constantly activate C2 and C4 in the plasma but C4b is rapidly inactivated because it does not bind to activating surface; for that reason, and because the concentrations of C2 and C4 are relatively low, no C3/C5 convertase is formed. Edema is caused by C2-kinin and bradykinin. 2.Which complement component levels will be decreased? Why? C2 and C4, because of the continous cleavage by activated C1.
Questionshereditary angioneurotic edema 3. Would you expect the alternative pathway components to be low, normal or elevated? C1 plays no part in the alternative pathway. This pathway is not affected. 4. What about the levels of the terminal components? The unregulated activation of the early components does not lead to the formation of the C3/C5 convertase, so the terminal components are not abnormally activated. 5. Despite the complement deficiency in patients with HANE, they are not unduly susceptible to infection. Why not? The alternative pathway of complement activation is intact and these are compensated for by the potent amplification step from the alternative pathway. 6. How might you decide the background of the laryngeal edema (HANO or anaphylactic reaction)? If the laryngeal edema is anaphylactic, it will respond to epinephrine. If it is due to HANO, it will not, C1INH needed.
Paroxysmal nocturnal hemoglobinuria (PNH) • Acquired clonal mutation of PIG-A gene in myeloid progenitors – no GPI-enchored proteins in the cell membrane of affected cells (rbc, plt, wbc) • CD59 and CD55 complement regulatory proteins are GPI-enchored proteins • No CD59 and/or CD55 PNH patients are highly susceptible to complement-mediated lysis • The lysis of red blood cells leads to high levels of hemoglobins in the blood that appears in the urine (hemoglobinuria) • Elevated levels of TF derived from complement-damaged leukocytes cause thromboses
Change in the colour of urine samples taken from PNH patient during the day
Haemolytic anaemia and associated symptoms Haemoglobin and its products in the urine Thrombosis: in brain veins, mesentheric veins, vv. hepaticae (Budd-Chiari-syndrome) Transformation to acut myelogenous leukemia (AML), aplastic anaemia, myelodisplastic syndrome (MDS) Specific th.: eculizumab (Soliris - anti-C5 monoclonal antibody) Curative th.: bone marrow transplantation Alternative th.: steroids (general immunosuppression) Anticoagulants: sc. heparin p.o. kumarin Iron replacement Transfusion (filtered-irradiated blood) Paroxysmal nocturnal hemoglobinuria (PNH) symptoms and therapy