Download
1 / 30
350 likes | 1.14k Views
BONE INFECTION MIMICKING BONE TUMORS: HOW TO MAKE THE DISTINCTION?. M. ATTIA, M. CHELLI BOUAZIZ, A. KAMMOUN , M F. LADEB. MUSCULOSKELETAL : MK 25 . INTRODUCTION.

E N D
BONE INFECTION MIMICKING BONE TUMORS:HOW TO MAKE THE DISTINCTION? M. ATTIA, M. CHELLI BOUAZIZ, A. KAMMOUN , M F. LADEB MUSCULOSKELETAL : MK 25
INTRODUCTION Bone infection often mimics bone tumors on imaging and clinical information is not always relevant for the diagnosis. An erroneous diagnosis may be responsible for delayed, ineffective or excessively mutilating treatments having severe consequences for the patient. The purpose of this presentation is to review the key elements for establishing a correct diagnosis of bone infection.
PATHOPHYSIOLOGY OF BONE INFECTION Bone infection may result from hematogenous spread, direct extension from a contiguous source or direct implantation and post surgery Osteomyelitis is the prototype of bone infection. Infective organisms present in the blood stream embolize in the sinusoidal vessels of the metaphysis. Septic venous thrombosis provokes interruption of endosteal and periosteal blood supply and secondarily bone necrosis If infection is not eradicated during the acute phase, subacute or chronic osteomyelitis can occur. This can be related either to inadequate therapy or to a specific host resistance to the infection.
Chronology of radiological changes D7 D15 D21 Normal Soft tissue swelling Demineralization Radiographs/CT Osteolysis Periosteal reaction MRI Abnormal bone marrow signal
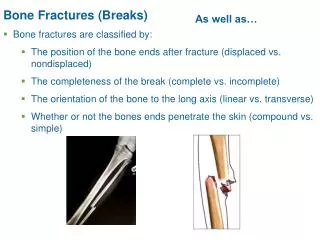
RADIOGRAPHS AND CT: OSTEOLYSIS Fig 1: Acute osteomyelitis of the humerus: ill defined osteolysis Ram PC et al. CT detection of intraosseous gas: a new sign of osteomyelitis. AJR 1981;137:721-723 Rafii M et al,. Hematogenous osteomyelitis with fat-fluid level shown by CT. Radiology 1984;153:493-494 Naidoo P. Extramedullary fat fluid level on MRI as a specific sign for osteomyelitis. Australas Radiol 2003;47:443-446 Fig 2: Activation of chronic osteomyelitis Transverse CT view of the tibia showing gas in the medullary cavity Results from inflammatory reaction and septic necrosis of bone trabeculae Most common in long bone metaphyses and diaphyses Presents as an ill defined radiolucent medullary area (Lodwick IC) (fig. 1) secondarily extending to the cortex in a moth eaten (Lodwick II) or permeative (Lodwick III) pattern CT provides a better analysis of trabecular and cortical bone osteolysis and may show non specific increased bone marrow density due to inflammatory infiltration. Presence of gas (fig. 2) or fat-liquid level in the medullary cavity is very specific of osteomyelitis in a non traumatic context.
RX AND CT MANIFESTATIONS: PERIOSTEAL REACTION Fig 3: Subacute osteomyelitis of the tibia. AP radiograph shows a well circumscribed lytic lesion with compact periosteal reaction A periosteal reaction is observed in half of acute, subacute or chronic osteomyelitis cases. It usually occurs early and is better diagnosed in children (fig. 3) It is detected earlier by CT rather than by radiographs Periosteal reaction may be unilamellar, plurilamellar or compact. However, it is not specific of osteomyelitis
RADIOGRAPHIC AND CT MANIFESTATIONS: SEQUESTRUM Fig 4: intracortical sequestrum in a patient with subacute osteomyelitis of the tibia. Note also the bone reaction surrounding the infection (involcrum) • The sequestrum is a devitalized bone fragment surrounded by granulation tissue. It is present in more than 50% of chronic osteomyelitis • It usually appears on radiographs as a condensed bone fragment with irregular margins and radiolucent rim (fig. 4) • The sequestrum is better detected by CT than by radiographs • The sequestum is characteristic of bone infection • However, the sequestrum is not absolutely specific of infection because it may be observed in histiocytosis, fibrosarcoma and may mimick a calcified osteoid osteoma nidus
RADIOGRAPHIC AND CT MANIFESTATIONS: SOFT TISSUE ABNORMALITIES • Radiographs and CT are relatively insensitive to soft tissue abnormalities • Ultrasound is the first method to diagnose subperiosteal or soft tissue collection • MRI allows an exhaustive study of bone and soft tissue • Soft tissue calcifications or ossifications are rare in musculoskeletal pyogenic infections and usually observed in tumors (osteosarcoma) and pseudotumors (myositis ossificans circumscripta). However, they are characteristic of musculoskeletal tuberculosis and may also be observed in hydatidosis or mycoses.
MRI FINDINGS: BONE MARROW EDEMA • MRI is very useful for the early diagnosis of musculoskeletal infection • In acute osteomyelitis, MRI typically shows low to intermediate T1 ( fig 5) and high T2 signal intensity areas involving the medullary canal the cortex and the soft tissues, corresponding to bone marrow edema Fig 5: Acute osteomyelitis of the distal tibia. Bone marrow edema of low T1 signal
MRI FINDINGS: BONE MARROW EDEMA • In subacute osteomyelitis, signal abnormalities are better circumscribed: intraosseous low T1 and high T2 signal intensity collections, sometimes containing a sequestrum of low T1 and T2 signal intensity (fig.6) • In chronic osteomyelitis, the bone shows a heterogenous signal associating low T1 and high T2 intensity areas (fluid) and low T1 and T2 areas (sclerosis). A B Fig 6: Bone sequestrum with periosteal reaction. CT(A) and T2 weighted MR (B) appearance
MRI FINDINGS: BONE MARROW EDEMA • Intravenous contrast administration enhances the periphery of bone collections and makes their detection easier (fig. 7) • Bone marrow edema is a sensitive but not specific sign of osteomyelitis. • Optional signs are more specific of this diagnosis • Fat globules • Penumbra • Double line
MRI FINDINGS: FAT GLOBULES Acute osteomyelitis causes septic necrosis of bone marrow Fat sediments with pus may resulting in intra or extra-osseous fat-liquid levels The presence of fat in acute osteomyelitis may result from either the persistence of normal bone marrow surrounded by edema or the presence of linear or globular foci of necrotic bone marrow (fig. 7) The presence of fat in soft tissues is an indirect sign of cortical disruption (fig. 8)
A B Figure 7 : Acute osteomyelitis of the humerus (same patient as fig 1). Note the presence of fat into the osteomyelitis focus on T1 weighted sequence (A). Bone and soft tissue collection are well depicted by IV Gadolinium administration (B).
A B Figure 8 : Subacute osteomyelitis of the distal femur: the presence of fat in the soft tissue (B) and the cortical sequestration (A) are very specific of bone infection.
MRI FINDINGS: PENUMBRA SIGN Figure 9 : Penumbra sign in a Brodie’s abcess of the proximal tibia. The abcess wall internal aspect shows a high signal on T1 weighted sequence (A) and after fat suppression and Gadolinium administration (B). Four concentric layers are observed on MRI (Fig 9): • the center (pus) has a low T1 and high T2 signal intensity • the internal ring (abcess wall) has an intermediate T1 and high T2 signal intensity • the external ring (reactional sclerosis) has low T1 and T2 signal intensity • the peripheral area (bone edema) has low T1 and high T2 signal intensity
MRI FINDINGS: PENUMBRA SIGN The penumbra sign (fig. 9) described on T1 weighted sequences corresponds to the relative hyperintensity of the internal ring compared to the other three layers Histologically, it corresponds to granulation tissue at the abcess wall (in bone, soft tissue or any other organ) This sign is specific of abcess (99%) but its sensitivity ranges from 27 to 75%
MRI FINDINGS: DOUBLE LINE SIGN Fig 10: Brodie’s abcess of the humerus. Transverse T2 weighted MRI shows a « double line » sign • The double line sign, described on T2 weighted sequences is less interesting . It corresponds to internal (hyperintense) and external (hypointense) rings (Fig 10). Its sensitivity is 22%
TUBERCULOUS OSTEITIS • Rare localization of musculoskeletal tuberculosis • Axial and appendicular skeleton • Pseudotumoral appearance • May be multifocal and mimick bone metastases Fig 12: tuberculous osteitis of the distal femur Fig 13: Tuberculous spondylitis. CT appearance Fig 10:Tuberculous osteitis of the ischium Fig 11: Tuberculous osteitis of the ilium. CT appearance
BONE HYDATIDOSIS • Parasitic infection caused by Echinococcus granulosus • Bone is rarely involved • It mainly occurs in thoracic spine, long bone localizations are rare • Radiographs and CT typically show a multiloculated lytic lesion with sometimes pseudotumoral pattern • Transarticular extension is possible • US and MRI: multicystic appearance
BRODIE ABSCESS Chronic osteomyelitis of the femur Osteoid osteoma of the glenoid process Brodie abscess is a form of subacute osteomyelitis manifesting as a focal bone lucency that may contain a sequestrum and be surrounded by bone sclerosis. It usually involves long bone metaphyses, typically the distal femur or proximal tibia. Periosteal reaction may be absent Differential diagnosis is the nidus of an osteoid osteoma that is a benign bone tumor occurring in children and young adults and presenting as a focal osteolysis (nidus), that may contain a central calcification, and peripheral bone sclerosis.
SUBACUTE OSTEOMYELITIS • Subacute osteomyelitis rarely presents as an isolated cortical hyperostosis. • In this case, differential diagnosis includes osteoid osteoma and stress fracture Subacute osteomyelitis of the tibia Osteoid osteoma of the femoral neck Stress fracture of the tibia
CHRONIC OSTEOMYELITIS • Chronic osteomyelitis occurs when acute osteomyelitis is insufficiently or inadequately treated. It usually manifests as a mixed lytic and sclerotic lesion. Moth eaten and permeative bone osteolysis, periosteal reaction and pathological fracture can also be observed • Diiferential diagnosis of these aggressive bone osteolysis patterns include osteosarcoma and Ewing tumor, which are malignant primitive bone neoplasms. Ewing Tumor of the fibula Chronic osteomyelitis of the humerus
BRODIE’S ABCESS • Brodie’s abcess usually presents on radiographs as a well circumscribed metaphyseal or metaphyso-epiphyseal lytic lesion surrounded by a sclerotic rim. Bone sequestrum and periosteal reaction may be absent • This radiographic pattern may be observed in giant cell tumor, and other benign or malignant bone tumors. In this example, telangiectasic osteosarcoma of the proximal tibia. Brodie’s abcess of the femur Telangiectasic osteosarcoma of the proximal tibia
CHRONIC OSTEOMYELITIS • mixed lytic and sclerotic bone appearance associated with periostal reaction may correspond either to chronic osteomyelitis or osteosarcoma. • In this case, MRI clearly depicted intra-osseous and soft tissue abcesses which allowed the diagnosis of chronic osteomyelitis Chronic osteomyelitis of the femur
BONE LYMPHOMA mixed lytic and sclerotic bone appearance associated with periostal reaction. doubt about the presence of a bone sequestrum on CT images. MRI clearly show intra-osseous and soft tissue involvement. Bone biopsy: bone lymphoma
TUBERCULOUS SPONDYLITIS Lateral radiograph and Sagittal CT image showing sclerotic collapsed thoracic vertebra. The presence of intrasomatic gas and péri-vertebral calcification are against tumor MRI show disc preservation and bilobed epidural abcess vertebral biopsy : tuberculous spondylitis
OSTEOSARCOMA • Osteosarcoma is a primitive malignant bone tumor occuring mainly in children and young adults. Radiographs may show osteolytic, sclerotic or mixed lytic and sclerotic pattern. • The differential diagnosis is chronic osteomyelitis. • In this case, the patient reported a two-year history of knee pain but inflammatory biological tests were negative. • Bone biopsy concluded at a conventional osteosarcoma Conventional osteosarcoma of the femur
CHRONIC OSTEOMYELITIS • Another example of chronic osteomyelitis mimicking primary bone tumor (Ewing Tumor). • In both cases, radiographs and CT show lytic and sclerotic bone appearance with soft tissue swelling. Ewing tumor of the ilium Chronic osteomyelitis of the ilium
CONCLUSION • Bone infection often mimics bone tumors on imaging • Clinical and biological information may be helpful but it is not always relevant for the diagnosis. • An accurate analysis of radiographic, CT and MRI signs may be very useful to establish a correct diagnosis because some signs are very specific and allow to differentiate both entities. • However, in some cases, positive diagnosis remains very difficult and bone biopsy is required.