Download
1 / 52

E N D
1. Chapter 20 The Heart
2. Heart Anatomy
3. Coverings of the Heart: Anatomy Pericardium � a double-walled sac around the heart composed of:
A superficial fibrous pericardium
A deep two-layer serous pericardium
The parietal layer lines the internal surface of the fibrous pericardium
The visceral layer or epicardium lines the surface of the heart
They are separated by the fluid-filled pericardial cavity
4. Coverings of the Heart: Physiology The pericardium:
Protects and anchors the heart
Prevents overfilling of the heart with blood
Allows for the heart to work in a relatively friction-free environment
5. Heart Wall Epicardium � visceral layer of the serous pericardium
Myocardium � cardiac muscle layer forming the bulk of the heart
Endocardium � endothelial layer of the inner myocardial surface
6. The Fibrous Skeleton 4 bands around heart valves and bases of pulmonary trunk and aorta that help stabilize valves & electrically insulate ventricular cells from atrial cells
Distribute forces of contraction
Add strength and prevent overexpansion of heart
Elastic fibers return heart to original shape after contraction
8. Internal Anatomy
9. Left and Right Ventricles
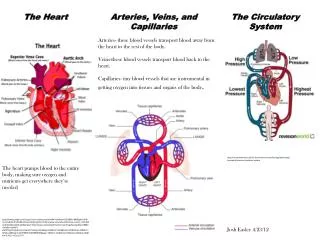
10. Pathway of Blood Through the Heart and Lungs Right atrium ? tricuspid valve ? right ventricle? pulmonary semilunar valve ? pulmonary trunk/arteries ? lungs? pulmonary veins ? left atrium ? bicuspid (mitral) valve ? left ventricle ? aortic semilunar valve ? aorta ? systemic circulation ? superior & inferior vena cavae ?right atrium
11. Cardiac muscle Microscopic anatomy
Striations (like skeletal mm)
Typically uninucleate
Fibers are short, branched and interconnected
Plasma membranes of adjacent cardiac cells interlock at intercalated discs
12. Intercalated discs Contain desmosomes
Anchor & prevent separation during contraction
Contain gap junctions
Allow ions to pass freely from cell to cell
Transmits depolarizing current across entire heart
Allows entire myocardium to behave like a functional syncytium
13. Cardiac Cells vs. Skeletal Fibers
14. Mechanism/events of contraction Automaticity or autorhythmicity
Some cardiac muscle cells are self-excitable
They can initiate their own depolarization
(and therefore the rest of the heart)
Remember�skeletal mm cells need to be independently stimulated by a nerve ending to contract
15. Organ vs motor unit contraction Gap junctions cause heart to contract as a whole or not at all via ion passage
Remember�in skeletal muscle all cells of a given motor unit contract together but not necessarily all motor units of a given muscle
16. Length of absolute refractory period Cardiac mm refractory period is 30x longer to prevent tetany which would stop the hearts pumping action
Cardiac cell contraction ~ 250 ms/refractory period~ 250 ms
Skeletal mm contraction ~ 20-100 ms/ refractory period~ 1-2 ms
17. Electrical events of cardiac cntrx 1-influx of Na changes membrane potential from �90 mV to ~+30 mV
2-depol travels thru T-tubules to cause Ca release from SR
3-Ca causes cross-bridge activation
Plateau results from Ca surge prolonging depol
This allows for sustained contraction needed to eject blood from the heart
18. Energy requirements Cardiac muscle has many more mitochondria
25% of cardiac cell volume
Compared to only 2% of volume in skeletal mm cell
High resistance to fatigue!
Relies almost exclusively on aerobic respiration
Cardiac muscles store oxygen in myoglobin
Cannot incur an O2 debt and still function normally
19. Electrical events of cardiac mm Intrinsic conduction
Non-contractile cardiac cells both initiate & distribute impulses causing depolarization in a sequential pattern allowing the heart to beat as a coordinated unit (functional syncytium)
Extrinsic conduction
SNS & PsNS
20. Intrinsic conduction Autorhythmic cells have an unstable resting membrane potential continuously drifting towards threshold for firing (called pacemaker potentials or prepotentials)
This mechanism is not fully understood but an influx of Ca instead of Na causes the rising phase of the action potential
21. Sequence of excitation of autorhythmic cells 1. Sinoatrial (SA) node�pacemaker
In Rt atrial wall (inf to Sup. Vena cava)
2. Atrioventricular (AV) node
Inf. Portion of interatrial septum above tricuspid valve
3. AV bundle (Bundle of His)
The only electrical connection b/t atria & ventricles & moderator band
4. Rt & Lt bundle branches
5. Purkinje fibers (in ventricular walls)
22. Impulse Conduction through the Heart
23. Arrhythmias Irregular heart beats/rhythms
Fibrillation � rapid, irregular, out-of-phase contractions
Ectopic focus � defective SA node where another part of the heart must assume its role
ie. AV node (junctional rhythm)
SA node is called �sinus rhythm
Extrasystole � premature contraction (b/f SA node initiates)
Heart block � damage to the AV node which inhibits the ventricles from receiving pacing impulses from the SA node
24. Extrinsic innervation SNS � increases both rate and force of contraction
PsNS � slows heart rate
Brain stem nuclei (in medulla oblongata)
Cardioacceleratory center
Cardioinhibitory center
25. Autonomic Pacemaker Regulation Rate of spontaneous depolarization depends on:
resting membrane potential
rate of depolarization
ACh (PsNS stimulation):
slows the heart
NE (SNS stimulation):
speeds the heart
26. Cardioacceleratory center Sympathetic center
Projects fibers to T1-T5 cord levels
Synapse in C & upper T SNS chain ganglia
Post-ganglionic fibers run thru the cardiac plexus to heart Parasympathetic center
Sends impulses to the dorsal vagus nucleus in the medulla oblongata
CN X sends (-) impulses to the heart
27. Electrocardiogram (ECG/EKG) 3 typical deflection waves
P wave (atrial depol) � 0.08 s.
QRS complex (vent. depol) � 0.08 s.
T wave (vent. repol) � 0.16 s.
Do not see atrial repol wave b/c it is hidden in the QRS complex
28. Typical EKG graph P-R interval � 0.16 s.
From atrial excitation to beginning of ventr. excitation
S-T segment
Entire vent. myocardium is depolarized
Q-T interval � 0.38 s.
From vent. depol thru vent. repol.
29. Holter monitor
30. Cardiac cycle All events assoc. w/ the flow of blood thru the heart during one complete heartbeat
Atrial systole (systole = contraction)
Atrial diastole (diastole = relaxation)
Ventricular systole
Ventricular diastole
Both sides pump same amount of blood with each beat
Pressure changes on the left side of the heart are ~5x greater than in the right�why???
31. Cardiac cycle terminology End diastolic volume (EDV)
Ventricles have max vol of blood in cycle
70% filling is passive/remaining 30% w/ atria contraction
Isovolumetric contraction phase
Vents begin to contract�AVs close/Semilunars not yet open (ventricles are �closed off completely�)
End systolic volume (ESV)
Remaining blood in vents after contraction
Isovolumentric relaxation phase
Chambers totally closed as remaining blood in great vessels flows backward to close semilunar valves
Dicrotic notch � brief rise in aortic pressure caused by backflow of blood rebounding off semilunar valves
32. Pressure and Volume in the Cardiac Cycle
33. Cardiac cycle time Assume 75 bpm
Cardiac cycle is ~0.8 s.
Atrial systole ~0.1 s.
Ventricular systole ~0.3 s.
Remaining 0.4 s. heart is in total relaxation
This is called the quiescent period
When heart rate increases:
all phases of cardiac cycle shorten, particularly diastole
34. Heart sounds Lub-dub, pause, lub-dub, pause�.
Lub � closure of AV valves�vent cntrx
Dub � closure of semilunar valves�vent relax
Pause � quiescent period
Murmurs:
Incompetent valves � backflow of blood
Normal vibration of thin heart walls
Children/elderly
35. AV Valve Function � �lub�
36. Semilunar Valve Function � �dub�
37. Cardiac output (CO=HR x SV) CO = volume of blood pumped by each ventricle in 1 minute
Stroke volume (SV) � amt of blood pumped with each beat
Cardiac reserve is the difference between resting and maximal CO
Ejection fraction is the percentage of EDV represented by the SV
38. Normal cardiac output HR ~ 75 bpm
SV ~ 70 ml/beat
CO = 75 x 70
CO = 5250 ml/min (5.25 L/min)
Adult blood vol ~ 5L�entire volume of blood passes through each side of the heart once each minute
39. Regulation of stroke volume SV = EDV-ESV
Normal SV ~ 70ml/beat�why?
EDV ~ 120 ml (length of diast + venous pressure)
ESV ~ 50 ml (arterial BP + force of vent cntrx)
�each ventricle pumps out ~ 60% of its volume w/ each heartbeat
40. 3 important factors affecting SV 1. Preload � amt vents are stretched by retained blood
Frank-Starling law of the heart
Stretching of heart mm cause max cross bridging� bigger force of contraction
2. Contractility � increase in contractile strength independent of mm stretch and EDV�extrinsic factors
Sympathetic stimulation
Hormones (glucagon, thyroxine,epi all stimulate)
Calcium and some drugs
3. Afterload � the pressure that blood must overcome for the ventricles to eject blood from the heart
41. Factors Affecting Stroke Volume
42. Vagal tone SNS & PsNS always maintain minimal stimulation to the heart with the PsNS being slightly more dominant
a vagotomy causes an immediate increase in RHR by~25 bpm
SA node has an inherent sinus rhythm of approx 80-100 bpm
AV node generates 40-60 AP�s/min
43. Bainbridge (atrial) reflex Baroreceptors notice increased dilation of atria from increased venous return & result in
1-direct SA node stimulation and
2-baroreceptor triggered (+) adjustments to SNS
leads to an increase in both HR and Force of contraction
44. Hormonal regulation of HR Epi/Norepi-(+) to rate & strength of contraction
Thyroxine- normally enhances BMR and body heat production
slower, more sustained increase in HR as compared to epi/norepi
45. Other factors w/ HR Age
fetus 140-160 bpm & declines w/ age
Sex
females 72-80 bpm
males 64-72 bpm
Heat
heat enhances metabolic rate of cardiac cells
cold decreases heart rate
Terms:
tachycardia - >100 bpm
bradycardia - <60 bpm
46. Coronary atherosclerosis
47. Coronary bypass
48. Congestive heart failure CO is so low that blood circulation cannot meet the needs of the tissues
usually progressive w/ various causes
coronary atherosclerosis
increase in aortic bp�increase in ESV�LV hypertrophy
MI�s lead to non-contractile scar tissue
dilated cardiomyopathy (DCM) - vents become flabby & ineffective
49. Left sided heart failure Pulmonary congestion
right side pumps to lungs but left side cannot accommodate returning blood�BV�s in lungs become engorged�pressure increases leaking fluid into tissues�pulmonary edema�person drowns (suffocates) Peripheral congestion
Left side pumps to body but right side cannot accommodate returning blood�blood stagnates w/in organs & tissues� cannot effectively exchange O2/wastes
edema is most noticeable in extremities (feet/ankles)
50. Developmental Aspects of the Heart By the end of the 3rd week:
The embryo has a system of paired vessels
The vessels forming the heart have fused
51. Development of Fetal Circulation Unique vascular modifications seen in prenatal development include umbilical arteries and veins, and three vascular shunts (occluded at birth)
Ductus venosus � venous shunt that bypasses the liver
Foramen ovale � opening in the interatrial septa to bypass pulmonary circulation
Ductus arteriosus � transfers blood from the right ventricle to the aorta
52. Circulation in Fetus and Newborn
53. Occlusion of Fetal Blood Vessels Umbilical arteries and vein constrict and become fibrosed
Fates of fetal vessels
Proximal umbilical arteries become superior vesical arteries and distal parts become the medial umbilical ligaments
The umbilical vein becomes the ligamentum teres
The ductus venosus becomes the ligamentum venosum
The foramen ovale becomes the fossa ovalis
The ductus arteriosus becomes the ligamentum arteriosum