Download
1 / 18
200 likes | 443 Views
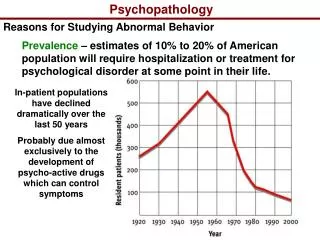
CHAPTER 16 DEVELOPMENTAL PSYCHOPATHOLOGY. Abnormality. Maladaptiveness Interferes with personal and social life Poses danger to self or others Personal distress DSM-IV diagnostic criteria (APA) Statistical deviance. Developmental Aspects. Development, not disease

E N D
Abnormality • Maladaptiveness • Interferes with personal and social life • Poses danger to self or others • Personal distress • DSM-IV diagnostic criteria (APA) • Statistical deviance
Developmental Aspects • Development, not disease • A pattern of maladaption, not defects • Social and Age Norms • Poor person-environment fit • Developmental Issues • Nature/Nurture • Risk factors • Prediction
The Diathesis-Stress Model • Interaction of genes and environment • Example: Depression • Genetic vulnerability • Environmental trigger(s) • Not specific stressors for specific disorders • “Bad things have bad effects for some people some of the time”
Autism • Begins in infancy, more boys • Several autistic spectrum disorders • Impaired social interaction, communication • Repetitive, stereotyped behaviors • 80% retarded: savant syndrome common • Severe cognitive impairment • Biologically based • Concordance: MZ=60%, DZ= 0%
Depression • Infancy • Somatic symptoms • Depressive-like states • Related to poor attachment • “At risk” if mother depressed • “Failure to thrive” syndrome may occur
Childhood • Externalizing Problems • “Undercontrolled” disorders • Acting out • Aggressive, out of control • Internalizing Problems • “Overcontrolled” disorders • Inner distress, shyness • More girls
Relationships between behavior at age 3 and psychological disorders at age 21. Part A shows that children with uncontrolled, externalizing behavioral styles are more likely than other children to show antisocial behavior and repeated criminal behavior at age 21. Part B shows that inhibited, internalizing children are at high risk of depression, but not anxiety disorders, at 21.
Attention-Deficit Hyperactivity Disorder • DSM-IV Criteria, some combination of the following: • Inattention, Impulsivity, Hyperactivity • More boys; 3-5% of US kids • Comorbidity common • Overactive behavior wanes with age • Attentional, adjustment problems remain • Most well-adjusted in adulthood
ADHD-Causes and Treatment • Neurological: Low Dopamine, other NT’s • Differential processing • Underactivity in motor area • Genetic predisposition; Environmental stress • 70% helped by stimulants (like Ritalin) • Overprescription a problem • Most successful if combined with behavioral treatment
Depression • Childhood • Somatic symptoms; school, social also • Psychotherapy, medication effective • Nature/Nurture question • Adolescence • Often related to childhood symptoms
Adolescence • Storm and Stress? • Only about 20% • Heightened vulnerability to psych disorders • Alcohol and drug problems • Eating Disorders • Anorexia nervosa; more girls (3/1) • Bulimia nervosa; binge-purge • Some genetic predisposition; stress also • Psychological treatment usually successful
Adolescent Depression and Suicide • 35% depressed; 7% diagnosable • Cognitive symptoms • Behavioral acting out • Genetic link • Environmental triggers • Suicide: Third leading cause of death • Males commit 3/1; girls attempt 3/1
Adulthood • Rates of disorder decrease after age 18 • Depression • Concern with elderly • Elderly less vulnerable to major depression • Depression often related to health • 15% have some symptoms • 1-3% diagnosable • Difficult to diagnose from otherconditions • More women (2/1)
Depression and Dementia • Many undiagnosed and untreated • Elderly can benefit, should NOT be excluded from treatment • Dementia: Progressive Deterioration • Not normal aging (Senescence) • Alzheimer’s Disease • Leading cause of dementia • Progressive and irreversible
Causes of Cognitive Impairment • Genetic: e.g., Alzheimer’s Disease • Vascular dementia-multi-infarct • Minor strokes: Deficits accumulate • Related to lifestyle: Diet and exercise • Reversible dementia, about 20% • Delirium: Reversible, often drug related • Depression: Treatable • Critical to distinguish for proper treatment
Alzheimer’s disease emerges gradually over the adult years; brain cells are damaged long before noticeable cognitive impairment results in old age. Changes in brain functioning are significantly different from those associated with normal aging.