
Enhancing Quality Measurement Strategies for Better Healthcare
E N D
Presentation Transcript
Cms quality programs University of North Carolina September 2019
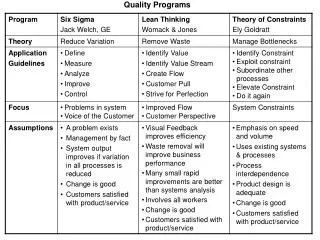
Quality Measurement What Makes a Good Quality Measure? (reliability, feasibility, validity, no unintended consequence, meaningful, impactful) Process of Measure Selection and Creation • Where do Measure Ideas get generated? • Conceptualization of a Measure • Development and Testing • Endorsement • Use in a Public Program • Assessment of Impact • Public Feedback • Harmonization For detailed information view Measure Blueprint
eCQM Strategy ProjectApproach to Learn Stakeholder Experiences
Transparency Transparency important so that patients have access to information to make best healthcare choices. Transparency has also engaged organizations in more quality improvement. Star ratings and transparency for patients • My Health e-data for patients • Nursing Home Compare • Hospital Compare • Physician Compare Price Transparency Quality Data Strategy • More rapid feedback to clinicians • API development for sharing quality data • Sharing data more broadly for research
Alignment One source of burden and confusion is that quality measures are not always aligned across all payers. CMS is engaged in multiple initiatives to promote alignment: • CQMC – Core Quality Measures Collaborative – between AHIP (Americas Health Insurance Plans), NQF and CMS to determine core ambulatory measures which can be agreed upon for ALL payers • Alignment efforts across CMS – Medicare FFS (traditional measures), Medicare Advantage, Medicaid, CMMI • Alignment efforts with VA and DOD per Presidential Executive Order • Alignment and efforts to review the CMS Measure Inventory (CMIT) to eliminate redundancies and measures with changed clinical evidence or measures that are topped out • Alignment efforts with QCDR (qualified clinical registries) to promote alignment and sharing of measures
Do We Need SDS Adjustment and if so, HOW? • Dual Eligible Status • Specific Risk Adjustment Factors • REL • Safety Net/DSH payments • Transportation • Food Availability • Literacy/Education • Community Characteristics (“stressed cities”)
QMVIG Value Based Programs Hospital Inpatient Quality Reporting Program Hospital Value Based Purchasing Program and Stars Program Hospital Outpatient Quality Reporting Program Ambulatory Surgical Centers Quality Reporting Program Inpatient Psychiatric Facility Quality Reporting Program ESRD Quality Incentive Program Hospital Acquired Condition Reduction Program Hospital Readmissions Reduction Program Merit Based Incentive Payment System (MIPS) Prospective Payment System for Exempt Cancer Hospital Quality Program Skilled Nursing Facility Value Based Program Home Health Quality Reporting Program Hospice Quality Reporting Program Inpatient Rehabilitation Facility Quality program Long Term Care Hospital Quality Reporting Program Promoting Interoperability – Hospital Program and Eligible Provider Program Marketplace – QRS Measure Set and Stars Program
Value Based Programs Update Hospital Stars • Stakeholder feedback that Stars program is difficult to understand, does not necessarily reflect true quality of a hospital • Public Comment Period • Recent NQF Summit • Upcoming Listening Session • New Technical Expert Panel • Rulewriting Process Current Plans • Refresh Stars in January 2020 under current methodology • Revised methodology January 2021 • Ongoing improvements Future: Listening Sessions and research on combined single/unified hospital program MIPS transformation to value
Provider Engagement: Quality Payment Program The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) requires CMS by law to implement an incentive program, referred to as the Quality Payment Program:
Merit-based Incentive Payment System (MIPS) Comprised of four performance categories So what? The points from each performance category are added together to give you a MIPS Final Score The MIPS Final Score is compared to the MIPS performance threshold to determine if you receive a positive, negative, or neutral payment adjustment Quick Overview MIPS Performance Categories 100 Possible Final Score Points = + + + Promoting Interoperability Improvement Activities Cost Quality
MIPS Year 4 (2020) Proposed Changes Performance Category Weights Year 4 (2020) Proposed Year 3 (2019) Final
MIPS Year 4 (2020) Proposed Changes Cost Performance Category Measures: Basics: Proposed:New episode-based measures and current global measures’ attribution methodologies revised Different measure attribution for individuals and groups
MIPS Year 4 (2020) Proposed Changes Payment Thresholds: *Payment adjustment (and exceptional performer bonus) is based on comparing final score to performance threshold and additional performance threshold for exceptional performance. To ensure budget neutrality, positive MIPS payment adjustment factors are likely to be increased or decreased by an amount called a “scaling factor.” The amount of the scaling factor depends on the distribution of final scores across all MIPS eligible clinicians.
MIPS Value Pathways CMS is proposing MIPS Value Pathways (MVPs) to create a new participation framework beginning with the 2021 performance year. This new framework would: Unite and connect measures and activities across the Quality, Cost, PromotingInteroperability, and ImprovementActivities performance categories of MIPS Incorporate a set of administrative claims-based quality measures that focus on population health/public health priorities Streamline MIPS reporting by limiting the number of required specialty or condition specific measures Request for Information
MIPS Value PathwaysGoal is alignment with specialty societies where feasible Current Structure ofMIPS (In2020) New MIPS Value PathwaysFramework (In Next 1-2Years) Future State ofMIPS (In Next 3-5Years) • Many Choices • Not MeaningfullyAligned • Higher ReportingBurden • Cohesive • Lower ReportingBurden • Focused Participation around Pathways thatare Meaningful to Clinician’s Practice/Specialty orPublic HealthPriority • Simplified • Increased Voice of thePatient • Increased CMS ProvidedData • Facilitates Movement to AlternativePayment Models(APMs) Building PathwaysFramework MIPS ValuePathways Clinicians report on fewer measures and activities baseon specialty and/or outcome within a MIPS ValuePathway Fully ImplementedPathways Continue to increase CMS provided dataand feedback to reduce reportingburdenonclinicians PromotingInteroperability Quality 6+ Measures 6+ Measures Moving toValue Value Quality ImprovementActivities Cost Cost ImprovementActivities 2-4 Activities 1 orMore Measures Foundation Promoting Interoperability Population Health Measures Enhanced Performance Feedback Patient-Reported Outcomes Foundation Promoting Interoperability Population Health Measures Population Health Measures:a set of administrative claims-based quality measures that focus on public health priorities and/or cross-cutting population health issues;CMS provides the data through administrative claims measures, for example, the All-Cause Hospital Readmissionmeasure. Cost Quality and IAaligned Goal is for clinicians to report less burdensome data as MIPS evolves and for CMS to provide more datathroughadministrative claims and enhanced performance feedback that is meaningful to clinicians andpatients. We Need Your Feedback on: Clinician/Group ReportedData CMS ProvidedData Pathways: What should be the structure and focus of the Pathways?What criteria should we use to select measures andactivities? Participation: What policies are needed for small practices and multi-specialtypractices?Should there be a choice of measures and activities withinPathways? PublicReporting: How should information be reported topatients? Should we move toward reporting at the individual clinicianlevel?
MIPS Value Pathways: Surgical Example Current Structure ofMIPS (In2020) New MIPS Value PathwaysFramework (In Next 1-2Years) Future State ofMIPS (In Next 3-5Years) MIPS moving towards value; focusing participation on specific meaningful measures/activities or public health priorities;facilitating movement to Advanced APMtrack Surgeon reports same “foundation” of PI andpopulation health measures as all other cliniciansbutnow has a MIPS Value Pathway with surgicalmeasures and activities aligned withspecialty Surgeon chooses from same set ofmeasures as all other clinicians,regardlessof specialty or practicearea Surgeon reports on samefoundationof measures with patient-reportedoutcomesalsoincluded Surgeon reports on fewer measures overall in apathway that is meaningful to theirpractice Four performance categories feel likefourdifferent programs Performance category measures in SurgicalPathway are more meaningful to thepractice MIPS Value Pathways forSurgeons Reporting burden higher andpopulationhealth not addressed CMS provides more data; reporting burdenonsurgeon reduced CMS provides even more data (e.g.comparative analytics) using claimsdataand surgeon’s reporting burden evenfurtherreduced QUALITYMEASURES IMPROVEMENT ACTIVITIES COSTMEASURES Unplanned Reoperation within the30-Day Postoperative Period (Quality ID:355) Use of Patient SafetyTools(IA_PSPA_8) Medicare Spending PerBeneficiary(MSPB_1) Clinician/GroupCMS Clinician/GroupCMS Clinician/GroupCMS Implementing the Use of SpecialistReports Back to Referring ClinicianorGroup to Close Referral Loop(IA_CC_1) Revascularization for LowerExtremityChronic Critical Limb Ischemia(COST_CCLI_1) Surgical Site Infection(SSI)(Quality ID:357) Knee Arthroplasty(COST_KA_1) Patient-Centered Surgical RiskAssessment andCommunication(Quality ID:358) OR Completion of an Accredited SafetyorQuality Improvement Program(IA_PSPA_28) *Measures and activities selected forillustrative purposes and aresubjecttochange. PromotingInteroperability Quality 6+ Measures 6+ Measures Quality ImprovementActivities Cost Cost Quality and IAaligned Cost ImprovementActivities Foundation Promoting Interoperability Population Health Measures Enhanced Performance Feedback Patient-Reported Outcomes Foundation Promoting Interoperability Population Health Measures 1 orMore Measures 2-4 Activities Population Health Measures: a set of administrative claims-based quality measures that focus on public health priorities and/or cross-cutting population health issues;CMS provides the data through administrative claims measures, for example, the All-Cause Hospital Readmissionmeasure.
MIPS Value Pathways: Diabetes Example Current Structure ofMIPS (In2020) New MIPS Value PathwaysFramework (In Next 1-2Years) Future State ofMIPS (In Next 3-5Years) MIPS moving towards value; focusing participation on specific meaningful measures/activities or public health priorities;facilitating movement to Advanced APMtrack Endocrinologist reports same “foundation” of PI and population health measures as all other clinicians but now has a MIPS Value Pathway with measures and activities that focus on diabetes prevention and treatment Endocrinologist chooses from same set of measures as all other clinicians, regardless of specialty or practice area Endocrinologist reports on same foundation of measures with patient-reported outcomes also included Endocrinologist reports on fewer measures overall in a pathway that is meaningful to their practice Four performance categories feel likefourdifferent programs Performance category measures in endocrinologist’s Diabetes Pathway are more meaningful to their practice MIPS Value Pathways forDiabetes Reporting burden higher andpopulationhealth not addressed CMS provides more data; reporting burden on endocrinologist reduced CMS provides even more data (e.g. comparative analytics) using claims data and endocrinologist’s reporting burden even further reduced QUALITYMEASURES IMPROVEMENT ACTIVITIES COSTMEASURES Hemoglobin A1c (HbA1c) Poor Care Control (>9%) (Quality ID: 001) Glycemic Management Services (IA_PM_4) Total Per Capita Cost (TPCC_1) Clinician/GroupCMS Clinician/GroupCMS Clinician/GroupCMS Chronic Care and Preventative Care Management for Empaneled Patients (IA_PM_13) Medicare Spending Per Beneficiary (MSPB_1) Diabetes: Medical Attention for Nephropathy (Quality ID: 119) Evaluation Controlling High Blood Pressure (Quality ID: 236) OR Electronic Submission of Patient Centered Medical Home Accreditation (IA_PCMH) *Measures and activities selected forillustrative purposes and aresubjecttochange. PromotingInteroperability Quality 6+ Measures 6+ Measures Quality ImprovementActivities Cost Cost Quality and IAaligned Cost ImprovementActivities Foundation Promoting Interoperability Population Health Measures Enhanced Performance Feedback Patient-Reported Outcomes Foundation Promoting Interoperability Population Health Measures 1 orMore Measures 2-4 Activities Population Health Measures: a set of administrative claims-based quality measures that focus on public health priorities and/or cross-cutting population health issues;CMS provides the data through administrative claims measures, for example, the All-Cause Hospital Readmissionmeasure.
Questions and comments Based on Your Questions
Accountable Care Organizations What is the patient understanding of ACO’s? What is the future of value based purchasing? What is the future of specialty quality programs?
Preparing for the Future of Value Based Care How Can QI Teams Prepare Clinics for Next Stages of Transformation to Value? How Can We Engage Clinicians in Quality Improvement – specifically using EHR? Comment: • Commitment to Continuous Learning and Continuous Quality Improvement – including trained in skills of QI (Lean, PDCA, High Reliability) • Data Analytic Systems and Support – needs to be at an individual physician level, easy to understand, tied to performance • Governance systems that support quality and CQI • Understanding of costs (very hard to do) • Engagement of, and listening to, customers (do you post individual pt. experience scores; are you tracking patient reported outcomes) • Transparency to patients – use of patient portal, Open Notes, Test results available immediately • Physician engagement in EMR – physician builders, participation with IT teams, assessment of individual’s use for efficiency (reduce burden)
Future Directions for CMS Transparency – Price Transparency, Quality Transparency, Performance Transparency Engaging Consumers – Compare Websites Engaging Governance Continued Pursuit of Value Based Models Interoperability Key Quality Areas: • Maternal Mortality • Pain Management/Substance Abuse/Opioids • Skilled Nursing Facility Safety • Healthcare Safety – High Reliability, Safety Events, Electronic Safety Reporting of Events, Diagnostic Error • Post Acute Care – alignment, frailty assessment
Questions Michelle.Schreiber@cms.hhs.gov