Download

1 / 37
420 likes | 712 Views
Nontuberculous Mycobacteria (NTM): Causes of Occupational & Environmental Lung Disease. Lee B. Reichman, MD, MPH Meet the Professor Turkish Thoracic Society 10 th Annual Conference April 25-29, 2007 Kemer, Antalya, Turkey. Objectives.

E N D
Nontuberculous Mycobacteria (NTM): Causes of Occupational & Environmental Lung Disease Lee B. Reichman, MD, MPH Meet the Professor Turkish Thoracic Society 10th Annual Conference April 25-29, 2007 Kemer, Antalya, Turkey
Objectives • Overview of spectrum of diseases caused by nontuberculous mycobacteria (NTM). • Overview of new / emerging NTM. • Discuss cases of occupational or environmental exposures and NTM disease. • Briefly review ‘new’ treatment options. • Discuss research needs.
Case • 52 y.o. pulp mill worker referred for evaluation of possible underlying occupational lung disease. • Abnormal chest radiograph and CT. • VATS biopsy + for AFB and noncaseating granulomas. • Microbiology: M. avium complex on lung culture. • Initial exam: Tachypneic. O2 with oximizer at 15 L/min; late inspiratory crackles.
Recovered fully when seen approximately 18 months later. Spirometry, lung volumes, and diffusing capacity normal. Mildly increased A-a gradient with maximal exercise.
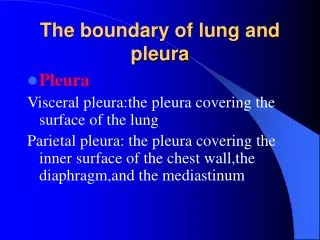
NTM: Spectrum of Disease • Pulmonary infections • Hypersensitivity pneumonitis • Skin and soft tissue infection • Lymphadenitis • Osteoarticular infections • Disseminated disease • Nosocomial infections
NTM: Pulmonary Infections -1 • Older men with pre-existing lung disease • COPD, ILD, bronchiectasis, prior TB • Cigarettes, alcohol, s/p gastrectomy, heart dz • Often upper lobe cavities • MAC and M. kansasii most common • Silico-mycobacteriosis
NTM: Pulmonary Infections -2 • Middle-aged & elderly women • RML and lingular bronchiectasis • Cystic fibrosis • Rapidly growing mycobacteria
Nontuberculous mycobacteria (NTM)Nomenclature • = ‘mycobacteria other than tuberculosis’ (MOTT) • [disease]= ‘atypical’ tuberculosis • Most common is M. avium complex • 61% of NTM isolates in U.S. • M. avium and M. intracellulare (MAI) • MAIS = MAI + M. scofulaceum • O’Brien R et al. ARRD 1987; 135:1007
Other NTM -1 • Rapidly-growing mycobacteria • 19% of NTM isolates in U.S. • O’Brien R et al. ARRD 1987; 135:1007 • More than 80% of clinical isolates are • M. abscessus • M. chelonae • M. fortuitum • Wallace RJ Jr., Clin Chest Med 1989:10:419
Other NTM -2 • M. kansasii: 10% of US isolates • Other NTM: remaining 10% • O’Brien R et al. ARRD 1987; 135:1007
NTM: Diagnosis -1 • Compatible symptoms & signs • Cough, fatigue; wt loss, dyspnea, fever, dyspnea • Exclusion of other diseases, e.g., TB, cancer • Radiography: CXR or HRCT • Infiltrates (> 2 mo or progressive), nodules, multifocal bronchiectasis, cavitation
NTM: Diagnosis -2 • Sputum: 3 positive cultures or 2 cxs and 1 smear OR • Bronchoscopy: single +cx or tissue bx + for AFB with one or more + cx (sputum or BAL) • Immunocompetent: > 2+ smear or growth • Immunosuppressed: 1+ or greater growth OR • Extrapulmonary: any + cx
The Older Older Man with MAC Photo courtesy of Michael Iseman, NJRMC
The Newer Older Woman with MAC Photo courtesy of Michael Iseman, NJRMC
Hot Tubs and Aerosol Exposures
Hot Tubs and Aerosol Exposures: Co-factors ?
Female sex No. (%) Mean age, yr (SD) Indoor hot tub, No. (%) Dyspnea Cough Fever Weight loss 20 (56%) 45 (16) 36 (100%) 35/36 (97%) 28/36 (78%) 21/36 (58%) 8/36 (22%) Hot Tub Lung Review - Marras TK et al. Chest 2005; 127
How It Really Happened • Family of 5 was quarantined for TB after work-up of wife/mother led to +AFB lung biopsy after 3 months of symptoms. • Astute public health MD suspected mis-diagnosis based on epidemiology and reviewed CT with colleague at National Jewish. HP was suggested. • Family members found profoundly ill in home. • Mangione EJ et al. EIDJ 2001; 7:1039
Showers as a Cause of MAC HP ? • 50-year-old male dentist had progressive exertional dyspnea and chest tightness for 3 months with 2-3 self-limited episodes of malaise, subjective fever, and myalgias, each lasting 24 to 72 h. • HRCT: small, bilateral, diffuse, centrilobular, ground-glass nodules & extensive mosaic attenuation consistent with air trapping on expiratory images • BAL: 53% lymphocytes. • Transbronchial biopsies: multiple well-formed nonnecrotizing granulomas, AFB stains negative. • Microbiology: Cultures from the BAL and two induced-sputa specimens grew MAC. • Marras TK et al. Chest 2005; 127:664
Environmental Studies • Hot tub filtered through swimming pool, both outside. Had not used hot tub for several weeks before symptom onset. Water cultures negative. • 3 of 4 water specimens from bathtub shower + for MAC. • No air sampling done. • Near-identical restriction patterns (0-1 band differences) for all respiratory and environmental isolates on pulsed-field gel electrophoresis, suggesting the strains were clonal. • No specific immunological data. • Authors concluded exposure must have been from showers. • Marras TK et al. Chest 2005; 127:664
Occupational Hypersensitivity Pneumonitis • Newly identified NTM species: M. immunogenicum • Shelton BG, Flanders WD, Morris GK. Mycobacterium sp. as a possible cause of hypersensitivity pneumonitis in machine workers. Emerg Infect Dis 1999; 5:270-273 • Moore JS, Christensen M, Wilson RW, et al. Mycobacterial contamination of metalworking fluids: involvement of a possible new taxon of rapidly growing mycobacteria. Am Ind Hyg Assoc J 2000; 61:205-213 • Respiratory illness in workers exposed to metalworking fluid contaminated with nontubeculous mycobacteria-Ohio, 2001. MMWR Morb Mortal Wkly Rep 2002; 51:349-352
Suggested Approach to Evaluation of Suspected NTM Disease -1 • High index of suspicion- clinical epidemiol • Occupational history: machinist; exposure to metal-working fluids? • Environmental history: hot tub? Indoor pools? • Confirm diagnosis with microbiology
Suggested Approach to Evaluation of Suspected NTM Disease -2 • CXR: ALWAYS review all serial films • HRCT: HP vs. infection • PFTs: serial FVC and DLCO • Oxygen needs assessment: desaturation?
NTM Evaluation - 3 • Industrial hygiene or environmental scientist consulation: Culture water, fluids and air in home/work. (Best to know your consultant.) • Communicate with microbiology laboratory: request PGFE or other fingerprinting method
NTM Evaluation - 4 • Remove from exposure or remove exposure from patient. • Treatment: anti-MAC vs. corticosteroids vs. both
Treatment of Pulmonary MAC Clarithromycin 500 bid or AZI 250 qd Rifampin 600 or Rifabutin 300 qd Ethambutol 25 mg/kg x 2 mos., then 15 mg/kg/day +/- (Streptomycin or) amikacin 2 or 3x/week x 2 months Treat until culture-negative for 12 months
American Thoracic Society Diagnostic Criteria of Nontuberculous Mycobacterial Lung Disease in HIV-Seropositive and HIV-Seronegative Hosts
Comparison of Clinicopathologic Forms of MAC Lung Disease -1
Comparison of Clinicopathologic Forms of MAC Lung Disease -2
Comparison of Clinicopathologic Forms of MAC Lung Disease -3
NTM Pulmonary Disease:Research Needs -1 • Data linking environmental exposures to NTM infection • Suspect indoor exposures more likely than outdoor: higher concentrations & more frequent. • Immunological responses to NTM • Markers of disease > exposure • Markers to distinguish infection & HP ? • Unusual opportunity in Queensland with Battey ag?
NTM Pulmonary Disease:Research Needs -2 • Risk factors for infection vs. HP • Are exposures really ubiquitous? Or are those affected exposed more? • If ubiquitous, what are susceptibility factors?
INFORMATION LINE 1•800•4TB•DOCS (482-3627) www.umdnj.edu/globaltb