Download
1 / 22
220 likes | 435 Views
Percutaneous Therapy of Pulmonic and Mitral Valve Disease. Atman P. Shah MD FACC FSCAI Director, Coronary Care Unit Assistant Professor of Medicine The University of Chicago February 4th, 2012. Disclosures. Consultant: St. Jude Medical, Abiomed, Medtronic Cardiovascular, Regenerx

E N D
Percutaneous Therapy of Pulmonic and Mitral Valve Disease Atman P. Shah MD FACC FSCAI Director, Coronary Care Unit Assistant Professor of Medicine The University of Chicago February 4th, 2012
Disclosures • Consultant: St. Jude Medical, Abiomed, Medtronic Cardiovascular, Regenerx • Speakers Bureau: Astra Zeneca, Medtronic, Novartis • NHLBI RO1 HL076671 2
Pulmonic Stenosis • Stenosis • Rheumatic inflammation • Supravalvular obstruction • Treatment if P-P >50mmHg • Size the balloon at 1.25 to annulus • Regurgitation • Treatment of Tetralogy • Congential malformation of valve • Associated with VSD, carcinoid, rheumatic involvement, trauma
Medtronic Melody Valve • 18, 20, 22 mm (28mm) via a 22 French size sheath
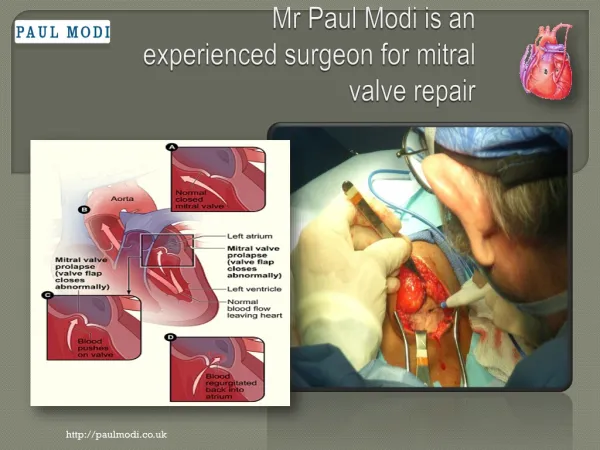
Perspective • >250,000 cases of significant Mitral Regurgitation diagnosed annually in the US • Current therapeutic options: • Medical management • Effective in symptom management • Ineffective in treating underlying pathophysiology or disease progression • Surgical Repair or Replacement (Standard of Care) • Effective yet invasive with associated morbidity • Only ~20% of patients with significant MR undergo MV surgery • Unmet need for an effective less invasive option 9 Investigational Device only in the US; Not available for sale in the US
Investigational Device only in the US; Not available for sale in the US Feldman et al. ACC.10
Investigational Device only in the US; Not available for sale in the US Feldman et al. ACC.10
Investigational Device only in the US; Not available for sale in the US Feldman et al. ACC.10
Investigational Device only in the US; Not available for sale in the US Feldman et al. ACC.10
EVEREST II RCT: Patient FlowPost MitraClip Procedure Acute Procedural Success Not Achieved n=41 Acute Procedural Success Achieved n=137 MV Surgery Post MitraClip Procedure n=9 2nd MitraClip Procedure n=2 2nd MitraClip Procedure n=3 No Additional Intervention n=11 MV Surgery Post MitraClip Procedure n=28 n=37 81% Follow-up 96% MR ≤2+ at 12 months 15 Investigational Device only in the US; Not available for sale in the US
Investigational Device only in the US; Not available for sale in the US Feldman et al. ACC.10
EII RCT: Safety & Effectiveness EndpointsIntention to Treat Cohort Safety Major Adverse Events 30 days Effectiveness Clinical Success Rate* 12 months Device Group, n=180 Device Group, n=175 15.0% 66.9% pSUP <0.0001 pNI =0.0005 Control Group, n=94 Control Group, n=89 47.9% 74.2% • Met non-inferiority hypothesis • Pre-specified margin = 25% • Observed difference = 7.3% • 95% UCB = 17.8% • Met superiority hypothesis • Pre-specified margin =2% • Observed difference = 32.9% • 97.5% LCB = 20.7% * Freedom from the combined outcome of death, MV surgery or re-operation for MV dysfunction >90 days post Index procedure, MR >2+ at 12 months LCB = lower confidence bound UCB = upper confidence bound 17 Investigational Device only in the US; Not available for sale in the US
Investigational Device only in the US; Not available for sale in the US Feldman et al. ACC.10
EVEREST II RCT: Summary • Safety & effectiveness endpoints met • Safety: MAE rate at 30 days • MitraClip device patients: 9.6% • MV surgery patients: 57% • Effectiveness: Clinical Success Rate at 12 months • MitraClip device patients: 72% • MV Surgery patients: 88% • Clinical benefit demonstrated for MitraClip System and MV surgery patients through 12 months • Improved LV function • Improved NYHA Functional Class • Improved Quality of Life • Surgery remains an option after the MitraClip procedure 19 Investigational Device only in the US; Not available for sale in the US
Conclusions • The treatment of pulmonic stenosis involves valvuloplasty with good long term results • Emerging technologies allow treatment of valvular disease previously thought to be only operable