Osteomyelitis
Osteomyelitis. Osteomyelitis. Hematogene verspreiding Verspreiding per continuitatum vanuit wekedelen of gewrichten Directe inoculatie t.g.v. trauma of chirurgie. Anatomic Classification. ( Cierny-Mader ) 1985. II:. III:. IV:. Hematogene osteomyelitis.


Osteomyelitis
E N D
Presentation Transcript
Osteomyelitis • Hematogene verspreiding • Verspreiding per continuitatum vanuit wekedelen of gewrichten • Directe inoculatie t.g.v. trauma of chirurgie
AnatomicClassification (Cierny-Mader) 1985 II: III: IV:
Acute osteomyelitis • Meestal in metaphyse • Doorbraak in gewricht septische artritis • Metaphyse in gewricht bij knie, heup en schouder
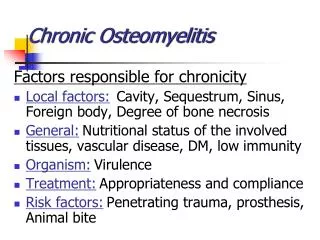
Chronische osteomyelitis • De aanwezigheid van een drainerende sinus is pathognomisch voor chronische osteomyelitis • Niet helende fracturen en Brodie’s abces • Diabetes mellitus • Ulcera onderliggende osteomyelitis • Als ulcer groter is dan 2 x 2 cm of bot is palpabel is de diagnose osteomyelitis zeer waarschijnlijk
Microbiology of osteomyelitis Mandell, Douglas and Bennett’s, Principles and practice of infectious diseases, seventh edition
Diagnostiek • Een accurate diagnose van osteomyelitis is cruciaal gezien de langdurige behandeling met antibiotica en de eventuele “aggressieve” chirurgische debridement.
Diagnostiek • Microbiologie • Pathologie • Beeldvorming: • Gewone röntgenfoto • MRI • Bot scan • PET CT Open chirurgisch biopt of naaldbiopsie
Beeldvorming • Op gewone x-foto zijn afwijkingen te zien 10 tot 14 dagen na de start van infectie
X-foto MRI Figure 1. Plain film radiograph of spinal discitis / osteomyelitis. Lateral view of the lumbar spine demonstrates L 3-4 disc space narrowing (arrow) and end-plate irregularity. Figure 2. MRI of lumbar spine discitis/osteomyelitis. A. Sagittal T1-weighted images of the lumbar spine in the same patient as figure 1 demonstrate T1-hypointense signal (solid arrows) centered around the L3-4 interspace. B. Post gadolinium sagittal fat-suppressed T1-weighted images shows marrow (dashed arrows) and disc enhancement with endplate erosions.
PET-CT An 11-y-old boy with history of X-linked chronic granulomatous disease who underwent 18F-FDG PET/CT as part of his work-up. Coronal PET image demonstrates several areas of osteomyelitis (both feet and distal right femur) (O), several soft-tissue sites of inflammation (left forearm, left femur, and both shins) (I), pneumonia (P), and paratracheal and hilar adenopathy (A). FDG = Fluorine 18 fluorodeoxyglucose
Microbiologie • Afname materiaal voor kweek • Open chirurgische biopsie • Naald biopsie • Bloedkweken
Speciale kweken • Mycobacterium tuberculosis • Schimmels en gisten • Brucella
Therapie • Chirurgische debridement • Plus eventueel: • Verwijderen van “hardware” • Revascularisatie • Complete sluiting wond (spierflap) • Stabiliteit waarborgen bij evt. fracturen • Antibiotica (langdurig) • Iv of oraal? Duur?
ZGV • Acute hematogene osteomyelitis:verwekker onbekendflucloxacilline, clindamycineverwekker bekendS aureus: flucloxacilline, clindamycineStreptokokken: peni, clindamycinePseudomonas: cefta + genta, cipro
ZGV • Na trauma of per continuitatemverwekker onbekendgeen perifere vaataandoeningFlucloxacilline, clindamycinewel perifere vaataandoeningclindamycine + /- cipro
Casus • Dhr R 52 jr. • Charcot osteoarthropathie voet • Ulcus met osteomyelitis • Bloedkweken: Streptococcus agalactiae • Wondkweek: Stapylococcus aureus HSC • Amoxicilline/ clavulaanzuur iv.
Kweken Bloedkweek Wondkweek
Vervolg casus • Allergie clindamycine • Vragen: • Is oraal behandelen mogelijk? • Welke orale opties zijn er? • Is er bewijs voor toegevoegde waarde van rifampicine?
Review CID CID 2012:54 (1 february)
Problemen chronische osteomyelitis • Geen goede representatieve kweken • Vaak “Delay” in behandeling • Therapiefalen
Parenterale antibiotica • Botpenetratie beta-lactams 5-20% serumspiegels • IV betalactam botspiegels > MIC • Orale dosering beta-lactam AB < 10% iv serumspiegels botspiegels < MIC
Parenterale antibiotica • Vancomycine lage penetratie in bot • Hoge serumspiegels botspiegels > MIC • Daptomycine idem.
Orale antibiotica • AB met goede penetratie in botweefsel: • Fluoroquinolonen ± 30-60% van serumspiegels • Linezolid ± 50% • Trimethoprim ± 50% • Sulfamethoxazol ± 10-20% • Doxycycline ± 2-86% afhankelijk welk bot • Clindamycine ± 40-70% • Metronidazol ± 80-100% • Rifampicine > 100% • Fusidinezuur ± 40-90% • Fosfomycine ± 25%
Gerandomiseerde studies AB behandeling chronische osteomyelitis • 8 kleine studies totaal N=228 • 5 studies vergelijken iv met oraal • Geen significante verschillen in uitkomst na 12 maanden • Bijwerkingen iv vs oraal 15,5% vs 4,8%
Rifampicine • 2 studies met toevoeging rifampicine bij chronische osteomyelitis S. aureus • Uitkomst beter in rifampicine groep • Genezing17 van 20 vs 12 van 21 • Zimmerli: geïnfecteerde prothesen • Cipro + rifamp vs cipro mono 3-6 mnd • Genezing 100% vs 58% • 4 van 5 pt met therapiefalen ontw. cipro R
Gerandomiseerde studies co-trimoxazol • Cloxacillin vs co-trim + rifamp bij S. aureus • N=50 • 8 weken • 20 patiënten met prothese • “Cure rate” 91% vs 89% • Follow-up 10 jr. “relaps rate” 10% vs 11%
Opmerkingen • Weinig hard bewijs bij AB behandeling chronische osteomyelitis • Studies met lage aantallen en heterogene groepen • Minder studies voor iv dan orale AB
Conclusies • Orale behandeling met oraal AB met goede penetratie bot lijkt acceptabel • Ciprofloxacine 2dd750mg • Co-trimoxazol 7-10 mg/kg/dg (trimethoprim) • Clindamycine, doxycycline, Linezolid • Toevoeging rifampicine alleen bewezen effect bij S. aureus • Geen evidence voor duur therapie (na chirurgische debridement)
Vervolg casus Bloedkweek Wondkweek
Behandeling? • Chirurgische debridement met sluiten defect mogelijk? • Beste orale optie co-trimoxazol? • Rifampicine toevoegen? • In 25% gevallen DM en osteomyelitis) toch amputatie… Vragen en discussie