
OVERVIEW
The effect of treating X-linked hypophosphatemic rickets on FGF23. Erik A. Imel M.D. 1,2 , Linda DiMeglio, M.D 2 , Siu L. Hui, Ph.D 1 , Thomas O. Carpenter, M.D. 4 , & Michael J. Econs M.D. 1,3

OVERVIEW
E N D
Presentation Transcript
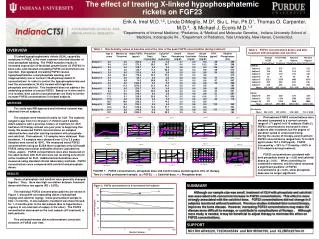
The effect of treating X-linked hypophosphatemic rickets on FGF23 Erik A. Imel M.D.1,2, Linda DiMeglio, M.D2, Siu L. Hui, Ph.D1, Thomas O. Carpenter, M.D.4, & Michael J. Econs M.D.1,3 1Departments of Internal Medicine; 2Pediatrics, &3Medical and Molecular Genetics, Indiana University School of Medicine, Indianapolis IN. , 4Department of Pediatrics, Yale University, New Haven, Connecticut Table 1: Biochemistry values at baseline and at the time of the peak FGF23 concentration during treatment OVERVIEW Table 2. FGF23 concentrations before and after treatment with phosphate and calcitriol X-Linked hypophosphatemic rickets (XLH), caused by mutations in PHEX, is the most common inherited disorder of renal phosphate wasting. The PHEX mutation results in increased expression of fibroblast growth factor 23 (FGF23) in bone cells, and elevated circulating FGF23 concentrations are reported. Dysregulated circulating FGF23 causes hypophosphatemia, renal phosphate wasting, and inappropriately low or normal 1,25-dihydroxyvitamin D concentrations. In order to control the hypophosphatemia and heal the osteomalacia, XLH is treated with high dose phosphate and calcitriol. This treatment does not address the underlying problem of excess FGF23. Based on in vitro and in vivo models, both calcitriol and phosphate are likely to further increase FGF23 concentrations in treated subjects. METHODS The study was IRB approved and informed consent was obtained from all subjects. Ten subjects were treated clinically for XLH. The subjects ranged in age from 2 to 30 years (7 children and 3 adults). Adult subjects with a previous history of treatment for XLH had been off therapy at least one year prior to beginning this study. We measured FGF23 concentrations on samples obtained before and after starting treatment with phosphate and calcitriol. Pretreatment, 1-3 samples were obtained. Post-treatment, 1-5 samples were obtained over 0.5 to 3.5 years. Samples were stored at -80ºC. We measured intact FGF23 concentrations using an ELISA that recognizes only full-length FGF23 using monoclonal antibodies (Kainos Laboratories, Tokyo, Japan). FGF23 concentrations were also measured on five adult women with XLH who were not receiving concurrent active treatment for XLH. Additional biochemistries were measured using standard clinical labsoratory methods. FGF23 concentrations were compared with calcitriol and phosphate doses. Pretreatment FGF23 concentrations were elevated (compared to a normal controls range of <71 pg/ml) in 9/10 subjects (Table 2). FGF23 concentrations increased in most subjects after treatment, but the degree of elevation varied in extent and timing. During the course of therapy, post-treatment FGF23 concentrations ranged from 74 to 3270 pg/ml (mean 767 ± 1059 pg/ml). FGF23 increased by > 20% in 7/10 and by >100% in 3/10 subjects during treatment. FGF23 concentrations correlated with both phosphate doses (p < 0.05) and calcitriol doses (p < 0.01). When controlling for combined treatment, calcitriol dose remained a significant predictor of FGF23 concentrations (p = 0.01), while phosphate dose was no longer significant. Subject 3 Subject 5 200 60 3500 70 180 3000 60 50 160 2500 50 140 40 120 2000 40 Phosphate mg/kg/d or FGF23 pg/ml Calcitriol ng/kg/d Phosphate mg/kg/d or Calcitriol ng/kg/d FGF23 pg/ml 100 30 Time in Months 1500 30 80 20 60 1000 20 40 10 500 10 20 0 0 0 0 0 6 12 18 0 6 12 18 24 30 36 42 Time in Months Subject 9 Subject 8 Subject 7 Subject 10 Subject 6 Medication stopped 2 months before last value Medication stopped one month before last value 1200 60 240 60.0 2200 60 230 60.0 300 60 2000 1000 50 235 50.0 50 1800 50 225 50.0 230 1600 800 40 40.0 40 200 40 220 40.0 1400 225 Phosphate mg/kg/d or Calcitriol ng/kg/d FGF23 pg/ml 600 30 Phosphate mg/kg/d or 1200 Calcitriol ng/kg/d Phosphate mg/kg/d or Calcitriol ng/kg/d Phosphate mg/kg/d or Calcitriol ng/kg/d FGF23 pg/ml FGF23 pg/ml FGF23 pg/ml Phosphate mg/kg/d or Calcitriol ng/kg/d FGF23 pg/ml 220 30.0 30 30 215 30.0 1000 400 20 215 800 100 20 20.0 20 210 20.0 600 210 200 10 400 10 10.0 10 205 10.0 205 200 0 0 0 0 200 0.0 0 0 200 0.0 0 6 12 18 24 30 36 42 48 FIGURE 1: FGF23 concentrations, phosphate dose and calcitriol dose plotted against time on therapy. Time 0 = initial pretreatment sample. ▲= FGF23, ■= Calcitriol dose, ●= Phosphate dose 0 6 12 18 24 0 3 6 0 6 12 18 24 0 3 6 Time in Months Time in Months Time in Months Time in Months Time in Months RESULTS Doses of phosphate and calcitriol were generally changed together. Thus, there was high correlation between treatment doses with these two agents (R2 = 0.873). The individual FGF23 concentration patterns are shown in Figure 1, along with corresponding doses of phosphate (mg/kg) and calcitriol (ng/kg). Initial pretreatment sample is time = 0 months. In two subjects, treatment was discontinued for 1- 2 months prior to the last sample (due to hypertensive urgency in one and lack of supply in the other). The FGF23 concentration decreased on the next sample (off treatment) in both patients. Five untreated women did not demonstrate consistent elevation of FGF23 over time. SUMMARY Although our sample size was small, treatment of XLH with phosphate and calcitriol was associated with concurrent increase in FGF23 concentrations. This effect is more strongly associated with the calcitriol dose. FGF23 concentrations did not change in 5 subjects monitored without treatment. Previous studies indicated that current therapy improves the bone disease. However, increasing FGF23 concentrations may make the disease more difficult to manage, or contribute to complications of therapy . Although more study is needed, it may be beneficial to adjust therapy to minimize the effect on FGF23 concentrations. SUPPORT NIH R01AR42228, T32DK065549 and MO1RR00750, and KL2RR025760-01





















