Download
1 / 1
10 likes | 140 Views
Childhood feeding problems are one of the most common developmental concerns seen by pediatricians (Silverman & Tarbell, 2010).

E N D
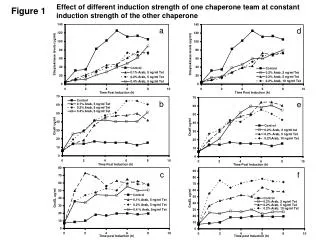
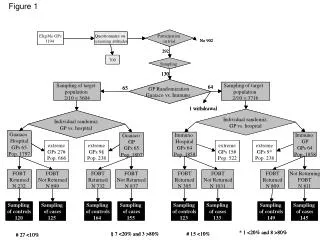
Childhood feeding problems are one of the most common developmental concerns seen by pediatricians (Silverman & Tarbell, 2010). Childhood feeding problems can be associated with a range of health problems (Kedesdy & Budd, 1998), as well as negative consequences for the child’s psychosocial functioning (Rommel et al., 2003). These severe effects on the child’s health and well-being often lead to increased stress and burden on the caregiver (Garro et al., 2005; Greer et al., 2008). There is however a paucity of research to suggest how a caregiver’s health-related quality of life (HRQOL) may be affected by a clinical feeding problem. Mothers of children with clinical feeding problems reported lower HRQoL than parents of children in the healthy community sample on the Total Summary Score, F(1, 450) = 41.635, p < 001; Parents Health-related Quality of Life Summary Score, F(1, 450) = 11.898, p < 001. There were no significant differences between groups on the Family Functioning Summary Score, F(1, 450) = 2.196, p = .139. The clinical feeding sample had significantly higher MBQ subscales scores for mealtime avoidance, F(1, 450) = 72.353, p < 001; food manipulation, F(1, 450) = 198.183, p < 001; and choking, gagging, and vomiting, F(1, 450) = 221.484, p < 001. Children with clinical feeding problems did not score significantly higher on the MBQ subscale of mealtime aggression, F(1, 450) = .071, p =.790. The Overall Effect of Childhood Feeding Problems on Caregiver’s Quality of LifeAmy J. Majewski1, W. Hobart Davies1, & Alan H. Silverman2University of Wisconsin-Milwaukee1 & Medical College of Wisconsin2 INTRODUCTION METHODS – MEASURES RESULTS • PedsQL™ Family Impact Module (FIM; Varni et al., 2004). The FIM is a 36-item measure used to assess parent HRQOL and family functioning. The measure generates 8 subscale scores (Physical, Emotional, Social, and Cognitive Functioning; Communication; Worry; Daily Activities; and Family Relationships), 2 Summary Scores (Parent HRQOL and Family Functioning), and a Total Score. Internal consistency is high across scales with Cronbach’s alphas ranging from α = .82 to α = .92. • Mealtime Behavior Questionnaire (MBQ; Davies et al., 2005). The MBQ is a 33-item parent-report measure used to assess problematic child behaviors at mealtime. The MBQ generates a total score from four subscales: Distraction/Avoidance, Food Manipulation, Mealtime Aggression, and Choking, Gagging, Vomiting. RESULTS Figure 2. MBQ Scores across Groups Figure 1. FIM Scores across Groups AIM OF PROJECT • This study aims to compare the HRQOL of parents of children with clinical feeding problems to parents of children within a healthy community sample. DISCUSSION and SUMMARY METHODS • Parents of children with feeding problems report lower HRQOL similar to families of children with other chronic conditions. • The current findings suggest that clinicians need to increase their awareness of how the parent is coping with their child’s feeding problem and ensure that they provide adequate support and resources for the parents. This will not only increase the overall well-being of the parent, but also may increase intervention success. • The stress and frustration related to the caregivers’ inability to effectively feed their child (Garro et al., 2005; Greer et al., 2008) may to be associated with deleterious effects on their overall health and well-being. • Although problematic mealtime behaviors are common across all children (e.g., aggression), it may be the frequency and severity of these problems that leads to significant problems with feeding (Crist & Napier-Phillips, 2001). • Due to the heterogeneous nature of feeding problems, further studies that examine the specific correlates of feeding problems may facilitate a better understanding of how individual disease-factors affect parent’s overall health-related quality of life. Clinicians may then be able to better identify and address the individualized needs and necessary supports that are unique to each family. • Participants • Participants were recruited from two different sites in order to utilize a clinical sample of parents of children with clinical feeding problems and a healthy community sample. • 452parents of young children completed questionnaires pertaining to their HRQOL and their child’s feeding habits. • Clinical Feeding Sample (n = 269) • Recruited from a large, Midwestern Children’s Hospital’s Interdisciplinary Feeding Clinic • Children diagnosed with clinical feeding problem. • Parents: • Age: M = 34.49, SD = 6.158 • 94.8% Female • 77.7% Caucasian • Community Sample (n = 183) • Recruited by undergraduate students at a large, Midwestern University as part of class credit. • Children with any history of chronic conditions were excluded from the sample. • Parents: • Age: M = 37.42, SD = 7.383 • 68.9% Female • 86.3% Caucasian Table 2. Means and Standard Deviations Note. ** denotes significant difference between group means, p < .05 Poster presented at the 2011 National Conference in Pediatric Psychology in San Antonio, TXCorrespondence for this project: Amy J. Majewski at amyjmajewski@gmail.com