Download
1 / 23
250 likes | 368 Views
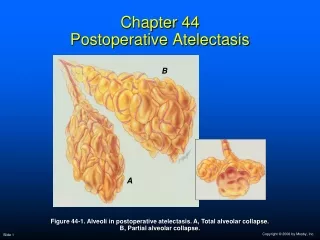
Chapter 44 Postoperative Atelectasis. B. A. B. A. Figure 44-1. Alveoli in postoperative atelectasis. A, Total alveolar collapse. B, Partial alveolar collapse. Anatomic Alterations of the Lungs. Alveoli of primary lobules (micro-atelectasis or subsegmental atelectasis)—very common

E N D
Chapter 44Postoperative Atelectasis B A B A Figure 44-1. Alveoli in postoperative atelectasis. A, Total alveolar collapse. B, Partial alveolar collapse.
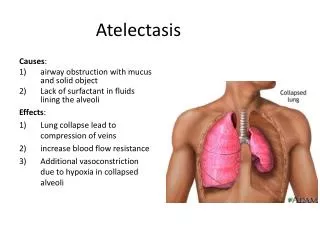
Anatomic Alterations of the Lungs • Alveoli of primary lobules (micro-atelectasis or subsegmental atelectasis)—very common • Lung segment—fairly common • Lung lobe—less common • Entire lung—rare
Etiology Decreased Lung Expansion • Thoracic and upper abdominal procedures • Considered high risk for atelectasis
Etiology Decreased Lung Expansion • Other precipitating factors • Anesthesia • Postoperative pain • Supine position • Obesity • Advanced age • Inadequate tidal volumes during mechanical ventilation • Malnutrition • Ascites • Diaphragmatic apraxia • The presence of a restrictive lung disorders
Etiology Alveolar Degassing Atelectasis associated with airway secretions and mucus plugs • Precipitating factors • Decreased mucociliary transport • Excessive secretions • Inadequate hydration • Weak or absent cough • General anesthesia • Smoking history • Gastric aspiration • Certain preexisting conditions (e.g., chronic bronchitis, asthma)
Overview of the Cardiopulmonary Clinical Manifestations Associated with POSTOPERATIVE ATELECTASIS The following clinical manifestations result from the pathophysiologic mechanisms caused (or activated) by Atelectasis (see Figure 9-7)—the major anatomic alterations of the lungs associated with postoperative atelectasis (see Figure 44-1)
Clinical Data Obtained at the Patient’s Bedside Vital signs • Increased respiratory rate • Increased heart rate, cardiac output, blood pressure
Clinical Data Obtained at the Patient’s Bedside • Cyanosis • Cough, sputum production, and hemoptysis • Chest assessment findings • Increased tactile and vocal fremitus • Dull percussion note • Bronchial breath sounds • Diminished breath sounds(when mucus plugs present) • Crackles • Whispered pectoriloquy
Figure 2-11. A short, dull, or flat percussion note is typically produced over areas of alveolar consolidation.
Figure 2-16. Auscultation of bronchial breath sounds over a consolidated lung unit.
Figure 2-19. Whispered voice sounds auscultated over a normal lungare usually faint and unintelligible.
Clinical Data Obtained from Laboratory Tests and Special Procedures
Pulmonary Function Study: Expiratory Maneuver Findings FVC FEVT FEF25%-75% FEF200-1200 N or N or N PEFRMVV FEF50% FEV1% N N or N N or
Pulmonary Function Study: Lung Volume and Capacity Findings VT RV FRC TLC N or VC IC ERV RV/TLC% N
Arterial Blood Gases Small or Localized Postoperative Atelectasis • Acute alveolar hyperventilation with hypoxemia pH PaCO2 HCO3- PaO2 (Slightly)
Time and Progression of Disease Disease Onset Alveolar Hyperventilation 100 90 Point at which PaO2 declines enough to stimulate peripheral oxygen receptors 80 70 60 PaO2 PaO2 or PaCO2 50 40 30 PaCO2 20 10 0 Figure 4-2. PaO2 and PaCO2 trends during acute alveolar hyperventilation.
Arterial Blood Gases Widespread Postoperative Atelectasis • Acute ventilatory failure with hypoxemia pH PaCO2 HCO3- PaO2 (Slightly)
Time and Progression of Disease Disease Onset Alveolar Hyperventilation Acute Ventilatory Failure 100 Point at which disease becomes severe and patient begins to become fatigued 90 Point at which PaO2 declines enough to stimulate peripheral oxygen receptors 80 70 PaCO2 60 50 40 30 PaO2 20 10 0 Figure 4-7. PaO2 and PaCO2 trends during acute ventilatory failure.
Oxygenation Indices QS/QT DO2 VO2 C(a-v)O2 Normal Normal O2ER SvO2
Radiologic Findings Chest radiograph • Increased density in areas of atelectasis • Air bronchograms • Elevation of the hemidiaphragm on the affected side • Mediastinal shift toward the affected side
General Management of Postoperative Atelectasis • Precipitating factors for postoperative atelectasis should be identified • High-risk patients should be monitored closely • Preventive measures should be prescribed for high-risk patients • Incentive spirometry • Chest physical therapy • Whenever possible, treatment of the underlying cause of atelectasis should be prescribed immediately
General Management of Postoperative Atelectasis Respiratory care treatment protocols • Oxygen therapy protocol • Bronchopulmonary hygiene therapy protocol • Hyperinflation therapy protocol • Mechanical ventilation protocol