Download
1 / 26
260 likes | 417 Views
Meg Pike & Justine Allan. Overview. Anatomy What is ITB Friction Syndrome? Signs & Symptoms Mechanism of Injury Rehabilitation Return to play Prevention of Reinjury. What is ITB Friction Syndrome?. Overuse injury Runners, Cyclists, Individuals who exercise vigorously

E N D
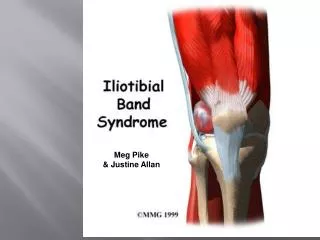
Meg Pike & Justine Allan
Overview • Anatomy • What is ITB Friction Syndrome? • Signs & Symptoms • Mechanism of Injury • Rehabilitation • Return to play • Prevention of Reinjury
What is ITB Friction Syndrome? • Overuse injury • Runners, Cyclists, Individuals who exercise vigorously • When ITB is tight or stressed it rubs against LFE more vigorously
ITB Anatomy • Originates: • Anterior Iliac Crest • Ilium • Iliac Spine • Gluteal muscles • Tensor Fascia Lata Muscle • Inserts: • Tibia • Patella • Biceps femoris tendon
Anatomical Clues • Tightness in hip adductors, iliopsoas, rectus femoris, gastrocemius and soleus • Weakness in hip abductors, especially gluteus medius • Overpronation • Lateral Pelvic Tilt • Leg Length discrepancies
Signs & Symptoms • Tenderness on lateral side of the knee • Pain triggered during flexion or extension of the knee • Crepitus • Could have pain in the hip • Pain aggravated by running and during activity, could progress to pain while walking
Mechanism of Injury • Repetitive knee flexion • Repeated running in one direction • Old running shoes • Running on the side of the road • Training Errors: “Too much too soon” • Increase in intensity or duration too quickly
Review: The Three Phases of Healing • Inflammatory Phase • 2-4 days • Acute Phase • Fibroblastic-Repair Phase • First few hours post-injury to 4-6 weeks • Subacute Phase • Maturation-Remodeling Phase • 3 weeks to several years • Recovery Phase
Rhonda Runners • 21 year old female cross country runner • Been running for 5 years, never injured before now • Hates stretching and experiences tight hamstrings and hip flexors • Loves running EVERY DAY! • After long runs she complains of pain and tightness in the right knee and clicking in the right hip • Wearing very old, out dated cross trainers • Over pronates
Rehabilitation Overview • Day 1 • Day 2 • Days 3-7 • Days 8-14 • Days 15-20 • Return to Sport
Day 1 • Injury Assessment • History • Observations • ROM • Palpations • Special Tests • Thomas Test (hip flexors) • Varus test (LCL) • Clark’s sign (PFS) • Nobel Compression (ITB) • Renee Creak Test (ITB) • Ober’s Test (ITB)
Day 1 (con’t) and Day 2 • Inflammatory (Acute) Phase • Cease injury-causing activity, curtail intensity of training program • PIER • NSAIDS • Acetaminophen • Ultrasound or electrical stimulation (IFC) for inflammation control
Ultrasound and IFC • Ultrasound • 3 MHz (superficial) • 50% or continuous intensity • 5 minutes • IFC • 80-150 Hz sweep pattern • 15 minutes
Days 3-7 • Inflammatory (Acute) Phase • Continue Rx for Days 1&2 if needed • Corticosteroids if needed • Glute/ITB roll if inflammation subsides • GOAL: to control/minimize inflammatory response
Days 8-14 • Fibroblastic-Repair (Subacute) Phase • Glute/ITB Roll (con’t) • Flexibility training: • Hip flexors (iliopsoas, RF/VI/VM/VL) • Hip extensors (gluteus maximus, BF/ST/SM) • Hip abductors (gluteus medius) • Hip adductors (adductor magnus/longus/brevis)
Days 15-20 • Fibroblastic-Repair (Subacute) Phase • Flexibility Training (con’t) • Myofascial therapy • Manipulative therapy • GOAL: Restore overall hip function, promote formation of healthy scar tissue
Day 21 • Maturation-Remodeling (Recovery) Phase • Strengthening exercises • Side-lying leg lifts (hip abductors) • Pelvic drops • Step-down exercises • GOAL: For the injured tissue to restore normal appearance and function.
Return to Sport • Return to sport/running: • Strength/stretches without pain • Easy sprints, even surfaces, every other day • Gradually increase distance and frequency • Most return to sport/running within 4-6 weeks.
Prevention of Reinjury • Maintain ROM and strength of hip muscles • Ensure adequate recovery between hard/fast training days • Avoid running on uneven surfaces • Wear proper shoes (attn: pronation/supination)