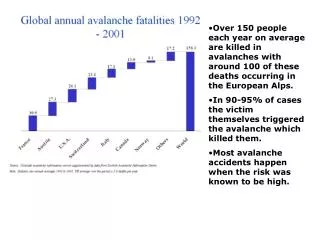
An estimated 3-5 million cases and over 100,000 deaths occur each year around the world.
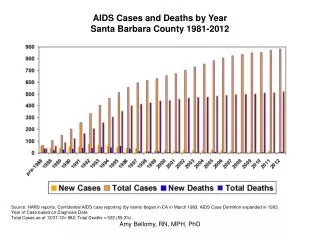
An estimated 3-5 million cases and over 100,000 deaths occur each year around the world. Since October 2010, over 470,000 Haitians have been sickened and nearly 7,000 have died.

An estimated 3-5 million cases and over 100,000 deaths occur each year around the world.
E N D
Presentation Transcript
An estimated 3-5 million cases and over 100,000 deaths occur each year around the world. Since October 2010, over 470,000 Haitians have been sickened and nearly 7,000 have died.
In 2011-2012-cholera outbreak in multiple African nations in all regions except north African regions-Ghana –due to intense hand washing campaign 30 May 2014-cholera outbreak –in sudan
CURRENT SITUATION • From October 2010 - Jan 2014,the govt. of Haiti has reported 698,304 suspected cholera cases and 8562 cholera related deaths • Of these,58,505 cases and 610 fatalities were recorded from Jan- december 2013 • Only 1396 cases and 16 fatalities have so far been registered in jan 2014 - reflecting significant reduction in number of cases
V.Cholerae - cholera • Name vibrio from latin as these bacteria possess single polar flagellum and appear to vibrate • Italian doctor Fillippo Pacini first discovered cholera bacillus in 1854 • Robert Koch first isolated in pure culture in 1883 • Causes cholera, acute watery diarrhea due to a potent Enterotoxin, disease of poor water sanitation
Epidemiology • Worldwide with epidemic, sporadic and pandemic nature • Poor sanitation, unsafe drinking water, natural calamities, overcrowding predispose. • 7 pandemics thus far • 6 originated in India - V.cholerae biotype classical, confined to Asia (1817 – 1923)
Epidemiology contd….) • 7th and current pandemic started outside India, 1961, in Indonesia by El Tor biotype • Humans are only sources of infection • Between periods of epidemics, bacteria survive in marine and estuarine water, zooplanktons
Genus Vibrio • Comprised of many species inhabiting fresh or marine water • Sensitive to acid pH but tolerate alkaline pH ( 8-9.6) very well • Curved Gram negative bacilli • Most important members are V.cholerae, V.parahemolyticus and V.vulnificus
Bacteriology • Curved Gram negative bacilli • Motile with single polar flagellum – DARTING MOTILITY • Facultative anaerobe and fermenter • Oxidase positive • Sensitive to acid pH but grows better at alkaline pH. • Humans are the natural hosts • Also found in marine and estuarine water
Antigens and classification • Possess somatic O antigen, flagellar H antigen and fimbrial antigen • O antigen and biochemical reactions are the basis of classification • 139 serovars ( O1 – O139), 2 biotypes( Classical and El Tor), 3 serotypes( Ogawa, Inaba, Hikojima) • V.cholerae O1 biotype ElTor is the common isolate now. • O139 isolation is also increasing
Classification- Gardner & Venkatraman V. cholerae O1 non O1 (O 2-139) Classical El Tor ogawa inaba hikojima
Virulence factors • Eneterotoxin – choleragen, an exotoxin 84kD protein with 2 domains. Resembles toxin of ETEC A domain is active, B domain for binding to intestinal epithelial cells(GM1 receptors) • Adhesins – fimbriae • Flagella • Mucinase & other proteolytic enzymes
Pathogenesis • Source: Patients and carriers • Vehicle of transmission: contaminated water and food, flies, fingers… • Mode of transmission: feco oral, ingestion • Incubation period : 1 – 5 days • Gastric acidity offers protection
Pathogenesis contd…) • Ingestion ( >106 bacilli) • Escape gastric acidity • Reach small intestine • Adhesion, colonisation, production of enterotoxin • Activation of adenyl cyclase • Overproduction of cAMP. • Outpouring of water & electrolytes into lumen • Watery diarrhea • Can secrete > 20L/Day • Dehydration
Pathogenesis cont.. • Addition ,multiplication, entrotoxin production (choleragen) • Choleragen (consists –A (active subunit) & B(binding subunit) • B subunit binds to ganglioside receptors-on surface of entrocytes • A subunit is inserted into cytosol
Catalyzes the addition of ADP-ribose to Gs protien (stimulatory G –protien) Locks the Gs protein in “ON” position Causes persistent stimulation of Adenylate cyclase Overproduction of CAMP stimulation-secretion of chlorine ion and water Leading-massive watery diarrhea- dehydration & electrolyte imbalance-death
Genes for cholera toxin and other virulence factor-carried on single stranded DNA bacteriophage –CTX Lysogenic conversion of non toxic producing strains to toxin producing one can occur-when CTX transduces these genes
1 2 Mechanism of Action of Cholera Toxin 3 4 NOTE: In step #4, uptake of Na+ and Cl- from the lumen is also blocked. HCO3- = bicarbonate which provides buffering capacity.
Pathology • Mucosa hyperemic, mild inflammation • NO INVASION, MUCOSA INTACT • Nature of stool: dilute , watery with mucus flakes – RICE WATER STOOL
Clinical features • Profuse watery diarrhea • May be upto 20L/day • Vomiting • Dehydration • No fever
Carrier state • Cholera is exclusively human disease • Infection mainly spreads from patient and carriers via contaminated water & food • There are’ NO’ known animal reservoirs and anthropod vectors • El Tor strain has got higher carriage state
3 types Incubator convalescent chronic Carrier Carrier Carrier Incubatorycarrier-shed vibrio only during brief period of incubation of cholera Convalescent carrier-in few cases bacilli may survive in gallbladder & excretion of vibrios may continue during convalescence -4-5 weeks
Chronic carrier-short , asymptomatic infection of gall bladder Found in endemic areas & vibrios are excreted in faeces intermittently from gall bladder El Tor cholera –greater incidence of casual carrier incidence rates- 7.3% in west bengal, 21.7% in philippines
Complications • Dehydration • Electrolyte imbalance • Hypovolemic shock • Death • Mortality 60% if untreated • 1% if adequately treated
LAB DIAGNOSIS • Specimen - Stool; Rectal swab. • Transport - VR medium; Cary Blair medium • Microscopy -For clinical purposes: darkfield or phase microscopic visualization of vibrios moving like‚ shooting stars‘, inhibited by serotype-specific antiserum • Gram stain- Comma shaped GNB • Culture - BA - small round moist colnies with heamodigestion • MA - late lactose fermenting • TCBS (selective ) - Yellow colored colonies ( Sucrose fermenter)
Identification: • String test +ve • Oxidase +ve; Catalase +ve • Cholera red reaction • Fermentation - Glucose, Sucrose, Mannitol • Confirmation: isolation of V. cholerae (serogroup 01 or 0139) from faeces, in non-epidemic areas final confirmation by biochemical and serologic reactions and detection of cholera toxin
Vibrio cholerae El Tor • 1st isolated in Celebes (Indonesia) in 1937-1938. • 7th Pandemic in 1960 – Honkong • 1963 – South west Pacific countries • 1970 – Africa • 1991 – South America
Treatment • Rehydration is essential: in severe cases, intravenous electrolyte solutions with alkali is used for initial stage, followed by oral rehydration; oral rehydration only may be used for mild cases • Formulation of ORS- Sodium chloride - 3.5g Potassium chloride - 1.5g Sodium citrate - 2.9g Glucose - 20.0g To be dissolved in 1 liter of clean drinking water
Appropriate antibiotics should be administered until the vibrio disappears from the stool Tetracycline or doxycyclineis useful –in reducing stool output in cholera & shortens period of excretion of vibrios
Preventive Measures Public Health Strategies Prevention comprises: • Basic sanitary and hygiene measures including • treated water supplies, improving water delivery and sewage control • adequate food hygiene • supplying handwashing facilities, latrines, boiled water • Prevention through immunization - considered as complementary to basic sanitary and hygiene measures
Vaccines - Complementary to sanitary and hygiene measures • Parenteral killed cholera vaccine, providing only partial protection (50%) of short duration (3-6 months), is not longer recommended • 2 newly developed oral vaccines have shown to be safe, immunogenic and effective, are licensed in some countries and are currently under consideration for use in public health: • Killed vaccine consisting of whole-cell V. cholerae O1 with purified recombinant B-subunit of cholera toxoid (WC/rBS) • Attenuated live vaccine based on the genetically modified V.cholera O1 strain‚ CVD 103-HgR‘
Cholera - Summary • Cholera no longer poses a threat to countries with minimum standards of healthy living but remains a threat for countries without access to safe drinking water and adequate sanitation • Proper treatment (rehydration!), reduces CFR <2% • Prevention is mainly based on basic sanitary and hygiene measures; newly developed oral vaccines are under consideration for their use in public health
NAG Vibrios • No agglutination with O 1 antisera • Can cause cholera like illness • O 139 Bengal - 1992 -1993; caused epidemic in Bangladesh & South east Asian countries
HALOPHILIC VIBRIOS • V.parahaemolyticus, V.alginolyticus, V.vulnifucus – marine habitat • V.parahaemolyticus: • Food poisoning due to ingestion of sea food • Vomiting, diarrhea, fever • Wound, eye & ear infections. • Kanagawa phenomenon – hemolysis in blood agar containing 7% NaCl and rabbit blood
V.alginolyticus: grows in 10% NaCl Otitis externa, marine wound infection cellulitis V.vulnifucus: Ferments lactose, capsulated, invasive Fatal wound infections & septicemia Gastroenteritis due to consumption of raw oysters
Aeromonas (Family Aeromonadaceae) • Gram-negative facultatively anaerobic bacillus resembling members of the Enterobacteriaceae • Motile species have single polar flagellum (nonmotile species apparently not associated with human disease) • 16 phenospecies: Most significant human pathogens A. hydrophila, A. caviae, A. veronii biovar sobria • Ubiquitous in fresh and brackish water • Acquired by ingestion of or exposure to contaminated water or food
Clinical Syndromes of Aeromonas • Associated with gastrointestinal disease • Chronic diarrhea in adults • Self-limited acute, severe disease in children resembling shigellosis with blood and leukocytes in the stool • 3% carriage rate • Wound infections • Opportunistic systemic disease in immunocompromised • Putative virulence factors include: endotoxin; hemolysins; eneterotoxin; proteases; siderophores; adhesins REVIEW
Plesiomonas • Formerly Plesiomonadaceae • Closely related to Proteus & now classified as Enterobacteriaceae despite differences: • Oxidase positive • Multiple polar flagella (lophotrichous) • Single species: Plesiomonas shigelloides • Isolated from aquatic environment (fresh or estuarine) • Acquired by ingestion of or exposure to contaminated water or seafood or by exposure to amphibians or reptiles • Self-limited gastroenteritis: secretory, colitis or chronic forms • Variety of uncommon extra-intestinal infections REVIEW