Download
1 / 15
150 likes | 304 Views
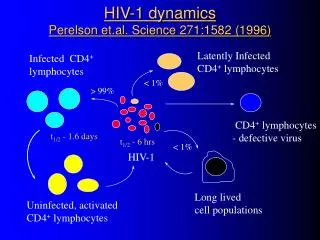
HIV-1 dynamics Perelson et.al. Science 271:1582 (1996). Latently Infected CD4 + lymphocytes. Infected CD4 + lymphocytes. < 1%. > 99%. CD4 + lymphocytes - defective virus. t 1/2 - 1.6 days. t 1/2 - 6 hrs. < 1%. HIV-1. Long lived cell populations. Uninfected, activated

E N D
HIV-1 dynamicsPerelson et.al. Science 271:1582 (1996) Latently Infected CD4+ lymphocytes Infected CD4+ lymphocytes < 1% > 99% CD4+ lymphocytes - defective virus t1/2 - 1.6 days t1/2 - 6 hrs < 1% HIV-1 Long lived cell populations Uninfected, activated CD4+ lymphocytes
Observations - viral dynamics • it takes 2.6 days to produce a new generation of viral particles • estimated total HIV production is 10.3 x 109 virions per day • at least 99% of the virus pool is produced by recently infected cells • retroviral therapy should be able to reduce viral load within a few days
HIV-1 RNA in plasma Mellors et.al. Science 272:1167 (1996) Pittsburgh cohort - 186 men enrolled in 1984/85 Baseline CD4 counts and plasma viremia were poorly correlated (r= - 0.27) CD4 counts are poorly predictive of disease progression and death HIV-1 RNA 0 600 1200 CD4+ cells
HIV-1 RNA in plasma Mellors et.al. Science 272:1167 (1996) Kaplan-Meier curves Baseline HIV-1 RNA < 4500 4500-13000 13000-36000 > 36000 1 0.5 Proportion surviving 0 There is a strong time- dependent prognostic relation between HIV-1 RNA and clinical outcome 0 5 10 Time (yrs)
HIV-1 RNA in plasma of neonatesShearer et.al. NEJM 336:1337 (1997) Prospective multicentre trial - 106 newborns Plasma HIV-1 RNA increased rapidly after birth and slowly declined over 24 months Infants with very high viral loads in the 1st month of life were at increased risk for rapid progression (p=0.006) rapid HIV-1 RNA nonrapid 0 12 24 Age - months
Receptors for HIV(Levy J. NEJM 1996;335:1529) HIV virus CD4 receptor is not enough for binding a Can manipulate these other receptors to prevent infection Genetic deletion of these receptors may explain why some individuals resist infection gp41 - gp120 Fusion CCR5 CD4 CXCR4 CELL SURFACE
Nucleoside analogues Zidovudine (AZT, ZDV) Zalcitabine (ddC) Didanosine (ddI) Stavudine (d4T) Lamivudine (3TC) Non-nucleoside reverse transcriptase inhibitors Protease inhibitors Saquinavir (Invirase) Ritonavir * (Norvir) Indinavir * (Crixivan) Nelfinavir * VX-478 * Nevirapine * Delavirdine * Loviride * Antiretroviral Agents * not approved in Canada
Combination therapy trialsACTG 175NEJM 335:1081 (1996) Methods • RCT- 52 centres & 2467 participants (CD4 200-500/mm3 • 4 treatment arms - ZDV vs ddI vs ZDV + ddI vs ddI + ddC • End points - >50 % decline in CD4; AIDS; death • Median FU 143 weeks - 565 reached an end-point Results • 32% of ZDV group reached endpoints compared to 18% ZDV + ddI (RHR 0.50); 20% ZDV + ddC (RHR 0.54); 22% ddI (RHR 0.64) • combination therapy appeared superior to monotherapy
Combination therapy trialsNuCombo(NEJM 1996;335:1099) Methods • RCT (21 sites and 1102 participants) • Men and women - CD4 counts < 200 / mm3 • 3 treatment arms (ZDV; ZDV + ddI; ddI + ddC) • End points - disease progression; death • Median FU 35 months - 64% reached an endpoint Results • 66% of ZDV group reached an endpoint compared to 62% of ZDV + ddI and 63% of ddI + ddC • No difference
Combination therapy trialsDelta Trial:Lancet 348:283 (1996) & 350:983 (1997) Methods • RCT -175 centres & 3207 participants (CD4 < 350 / mm3) • 3 treatment arms (ZDV vs. ZDV + ddI vs. ZDV + ddC) • End points - AIDS; death • Median FU 30 months - 51% reached an endpoint Results • 26% ZDV group reached an endpoint compared to 18% ZDV + ddI (RHR 0.67); 21% ZDV + ddC (RHR 0.79); • A greater effect was found in those without previous ZDV • High rates of early ZDV resistance in all groups
Protease inhibitor trial Hammer et.al, ACTG 320 NEJM 337:725 (1997) Methods • RCT (40 sites & 1156 participants) • CD4 counts < 200 / mm3 & previous ZDV therapy • RCT - 2 arms (ZDV + LAM vs ZDV + LAM + Indinavir) • End points - AIDS; death • Median FU 38 weeks - only 8% reached an endpoint Results • 6% IND group reached an endpoint compared to 11% ZDV + LAM (RHR 0.5, 95% CI 0.3-0.8) • The CD4 & HIV-RNA responses paralleled clinical results • Indinavir useful in late disease
Protease inhibitor trialGulick et.al. NEJM 337:734 (1997) Methods • RCT (97 participants) with previous ZDV therapy • CD4 - 50 to 400/ mm3 & >20,000 copies of HIV RNA/ml • 3 arms (INDINAVIR vs ZDV/ LAM vs IND/ ZDV/LAM) • End points - CD4; ¯ HIV RNA • FU 24 weeks (terminated early) Results • ZDV/LAM - no change in HIV-RNA or CD4 & 84% resistance to LAM • IND alone - initial ¯ HIV RNA & 53% resistance • 3 drugs - sustained ¯ HIV RNA & CD4 (16% resistance)
Principles of therapy • monitor plasma viral load and CD4 • initiate treatment before immunodeficiency becomes apparent • aim to reduce plasma viral load to undetectable levels • use combination of at least 2 drugs • change to a new combination if plasma viral load rebounds despite continued therapy
Problems with therapy • limited availability • very expensive (3 drugs ~ $25,000 / yr) • poorly tolerated - reduced compliance • multiple drug interactions • viral resistance - occurs in both exposed and non-exposed individuals • data from clinical trials very limited
Therapy recommendations (IAS-USA 1997) • Preferred: 2 nucleoside analogues plus a protease inhibitor example: ZDV + ddI + indinovir • Alternative 1: 2 nucleoside analogues + non-nucleo. RT inhibitor example: ZDV + 3TC + nevirapine • Alternative 2: 2 nucleoside analogues example: ZDV + ddI or 3TC + d4T • Not recommendedany monotherapy