Download
1 / 11
140 likes | 319 Views
Cell Signaling . Lecture 10. Receptor Tyrosine Kinases. Regulate cell proliferation, differentiation, cell survival and cellular metabolism The signaling molecules that activate RTK are soluble or membrane bound peptide or protein hormones Examples; Nerve growth factor (NGF)

E N D
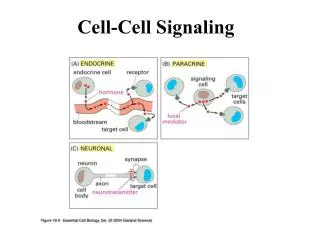
Cell Signaling Lecture 10
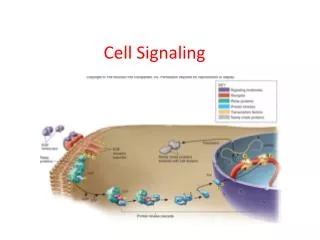
Receptor Tyrosine Kinases • Regulate cell proliferation, differentiation, cell survival and cellular metabolism • The signaling molecules that activate RTK are soluble or membrane bound peptide or protein hormones • Examples; Nerve growth factor (NGF) • Platelets-derived growth factor (PDGF) • Fibroblast growth factor (FGF) • Epidermal growth factor (EGF)
Like cytokine receptors, RTK signal through a protein tyrosine kinase • Unlike cytokine receptors, which associate with a separate cytosolickinase protein (JAK), RTKs have an intrinsic kinase as part of their cytosolic domain
Ligand Binding Leads to Autophosphorylation of RTKs • All RTKs comprise an extracellular domain containing a ligand-binding site, a single hydrophobictransmembraneα helix, and a cytosolic domain that includes a region with protein-tyrosine kinase activity. • Binding of ligand causes most RTKs to dimerize; • the protein kinase of each receptor monomer then phosphorylates a distinct set of tyrosine residues in the cytosolic domain of its dimer partner, a process termed autophosphorylation. • Autophosphorylation occurs in two stages. • First, tyrosine residues in the phosphorylation lip near the catalytic site are phosphorylated. • This leads to a conformational change that facilitates binding of ATP in some receptors (e.g., the insulin receptor) and binding of protein substrates in other receptors (e.g., FGF receptor). • The receptor kinase activity then phosphorylates other sites in the cytosolic domain; the resulting phosphotyrosines serve as docking sites for other proteins involved in RTK-mediated signal transduction.
Types of RTK • HER1: EGF, HB-EGF, TGFα • HER2: does not directly bind a ligand, forms heterodimers with ligand-bound HER1, HER3, HER4 • HER3: Neuregulins 1 and 2 (NRG), lacks a functional kinase domain and can signal only when complexed with HER2 • HER4: NRG1, NRG2, HB-EGF
Down-regulation of RTK Signaling • Endocytosis and Lysosomal Degradation • Overexpression of HER2 occurs in breats cancer
Further reading • http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2914105/
Abstract writing (Slamon et al., 2001) • BACKGROUND: • The HER2 gene, which encodes the growth factor receptor HER2, is amplified and HER2 is overexpressed in 25 to 30 percent of breast cancers, increasing the aggressiveness of the tumor. • METHODS: • We evaluated the efficacy and safety of trastuzumab, a recombinant monoclonal antibody against HER2, in women with metastatic breast cancer that overexpressed HER2. We randomly assigned 234 patients to receive standard chemotherapy alone and 235 patients to receive standard chemotherapy plus trastuzumab. Patients who had not previously received adjuvant (postoperative) therapy with an anthracycline were treated with doxorubicin (or epirubicin in the case of 36 women) and cyclophosphamide alone (138 women) or with trastuzumab (143 women). Patients who had previously received adjuvant anthracycline were treated with paclitaxel alone (96 women) or paclitaxel with trastuzumab (92 women). • RESULTS: • The addition of trastuzumab to chemotherapy was associated with a longer time to disease progression (median, 7.4 vs. 4.6 months; P<0.001), a higher rate of objective response (50 percent vs. 32 percent, P<0.001), a longer duration of response (median, 9.1 vs. 6.1 months; P<0.001), a lower rate of death at 1 year (22 percent vs. 33 percent, P=0.008), longer survival (median survival, 25.1 vs. 20.3 months; P=0.01), and a 20 percent reduction in the risk of death. The most important adverse event was cardiac dysfunction of New York Heart Association class III or IV, which occurred in 27 percent of the group given an anthracycline, cyclophosphamide, and trastuzumab; 8 percent of the group given an anthracycline and cyclophosphamide alone; 13 percent of the group given paclitaxel and trastuzumab; and 1 percent of the group given paclitaxel alone. Although the cardiotoxicity was potentially severe and, in some cases, life-threatening, the symptoms generally improved with standard medical management. • CONCLUSIONS: • Trastuzumab increases the clinical benefit of first-line chemotherapy in metastatic breast cancer that overexpresses HER2.
Abstract 2, Adedayo et al., 2009 Objective: To compare the clinicopathologic features and survival in the four breast cancer subtypes defined by immunohistochemistry (IHC) expression of estrogen receptor (ER) or progesterone receptor (PR) and human epidermal growth factor receptor 2 (Her2): ER/PR+,Her2+; ER/PR+, Her2-; ER/PR-,Her2+; and ER/PR-,Her2-. Methods: A 7-year retrospective study of 1134 invasive breast cancer subjects. Clinical and pathologic features and survival of the four subtypes were compared. Results: Using ER/PR+ and Her2- as a reference, ER/PR-,Her2- had the worst overall survival (hazard ratio, 1.8; 95% confidence interval [CI], 1.06-3.2) and the worst disease-free survival (hazard ratio, 1.5; 95% CI, 0.8-3.0). In ER/PR+,Her2-, chemotherapy conferred significant overall and disease-free survival advantages. Subtype comparison revealed statistically significant differences in outcomes. Conclusion: The triple negative subtype has the worst overall and disease free survival. Efforts should be directed at standardization of current testing methods and development of more reliable and reproducible testing.
Abstract 3, Slamon et al., 1989 Carcinoma of the breast and ovary account for one-third of all cancers occurring in women and together are responsible for approximately one-quarter of cancer-related deaths in females. The HER-2/neu proto-oncogene is amplified in 25 to 30 percent of human primary breast cancers and this alteration is associated with disease behavior. In this report, several similarities were found in the biology of HER-2/neu in breast and ovarian cancer, including a similar incidence of amplification, a direct correlation between amplification and over-expression, evidence of tumors in which overexpression occurs without amplification, and the association between gene alteration and clinical outcome. A comprehensive study of the gene and its products (RNA and protein) was simultaneously performed on a large number of both tumor types. This analysis identified several potential shortcomings of the various methods used to evaluate HER-2/neu in these diseases (Southern, Northern, and Western blots, and immunohistochemistry) and provided information regarding considerations that should be addressed when studying a gene or gene product in human tissue. The data presented further support the concept that the HER-2/neu gene may be involved in the pathogenesis of some human cancers.