Download
1 / 41
410 likes | 473 Views
Learn about IMCI strategy in Palestine to improve child health, reduce mortality, and enhance growth and development. Explore the components, objectives, and benefits of IMCI in the Palestinian context.

E N D
PalestineMOH Integrated Management of Childhood Illness: The road to healthy childhood Palestinian Experience in IMCI Dr. Younis Awad Allah IMCI National Coordinator MPH
Family is the unit of the community Child is the heart of the family Children are the future
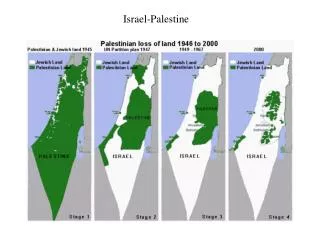
Palestine • Total population in OPT: 3,762,005 West Bank: 2,372,216 Gaza Strip: 1,389,789 • , Proportion of pop aged under 5 years (19.2% in GS and 16.6% in WB) • Reported CBR per 1000 pop (33.7 in GS Vs 23.9 in WB) • Reported CDR per 1000 pop (3.1 in GS Vs 2.5 in WB) • IMR 20.8 per 1000live births( 20.8 in GS Vs 3.9 in WB). • Child U5years mortality rate 20.07 per 1000 live births (24.6 in GS Vs16.3 in WM
Child Health care • The Palestinian authority has recognized child survival interventions as a high priority since long time . • Many child health care interventions were introduced during the last period, commonly run through vertical national programme . CDD and ARI programs were adopted since 1994. • EPI programme passing with an excellent coverage • Breastfeeding and supplementary feeding programme need more activation . • Screening of newborns for hypothyroidism and PKU still active programme. • WBC and anthropometric measures programme need more activation.
What Is Integrated Management of Childhood Illness IMCI • The united Nation “Convention on the rights of child” urge countries to take appropriate measures to fully implement the rights of child ;among which are: • 1- to diminish infant and child mortality; • 2- to ensure the provision of necessary medical assistance and health care to all children with emphasis on development of primary health; • 3- to combat diseases and malnutrition; • 4- to ensure that parents and children have access to education and are supported in the use of knowledge of child health and nutrition.
World challenge • WHO estimate that about 12 million children in developing countries die every year before reaching their fifth birthday. • Seven in 10 of these deaths are due to one or combination of group of common diseases. These are ARIs (mostly pneumonia), dehydration (due to diarrhea) ,measles, malaria and malnutrition. • In addition, one, or a combination of these five condition causes 3 in 4 episodes of childhood illness.
Bryce J, et al. “WHO estimates of the causes of death in children.” Lancet 2005.
So; WHO, CHD, with UNICEF responded by developing the strategy known as IMCI
IMCI Strategy • IMCI is neither another vertical program, nor a project, it is astrategy of managing common illnesses among children under -5years of age.
Recently WHO (EMRO) Announcement (Nov.2007) • IMCI is adopted by the Regional Office as the primary child health care strategy, offering a wide range of interventions under its overall umbrella and countries invited to see IMCI within this vision, and not as a vertical training program, and to commit increased resources for it to achieve the child mortality-related Millennium Development Goal no. 4.
IMCI Objectives • 1- To reduce significantly mortality and morbidity associated with the major causes of disease in children. • 2- To contribute to healthy growth and development of children.
Pneumonia Diarrhea Measles Malaria Malnutrition Sepsis Meningitis Dehydration Anemia Ear infection HIV/AIDS Wheezing Sore throat IMCI Addresses Most Causes of Death
Integrated Management of Childhood Illnesses (IMCI) • integrated approach • aims to reduce death, illness and disability, and to promote improved growth and development • includes both preventive and curative elements • implemented by families, communities and health facilities
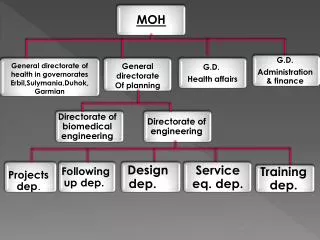
Components of IMCI The IMCI strategy seeks to reduce the child mortality through a broad and cross-cutting approach with components as: • Improves health worker skills • Improves health systems • Improves family and community practices
Clinical Assessment and treatment by health workers Knowledge, Beliefs and skills caretakers Capacity, structure and functions of health system Improving Health Worker Skills, Community Care, and Health Systems
IMCI as a Key Strategy for Improving Child Health Strengthening health workers skills Strengthening health system support Strengthening community involvement & participation Integrated Management of Childhood Illness Strengthening health workers skills Strengthening health system support Strengthening community involvement & participation
IMCI as a Key Strategy for Improving Child Health Strengthening health workers skills Strengthening health system support Strengthening community involvement & participation Integrated Management of Childhood Illness Strengthening health workers skills Strengthening health system support Strengthening community involvement & participation
IMCI as a Key Strategy for Improving Child Health Strengthening health workers skills Strengthening health system support Strengthening community involvement & participation Integrated Management of Childhood Illness Strengthening health workers skills Strengthening health system support Strengthening community involvement & participation
IMCI as a Key Strategy for Improving Child Health Strengthening health workers skills Strengthening health system support Strengthening community involvement & participation SICK CHILD Integrated Management of Childhood Illness WELL CHILD Strengthening health workers skills Strengthening health system support Strengthening community involvement & participation
Introduction of IMCI was significantly associated with: • reductions in the misuse of antibiotics A simplified model of IMCI impact • Correct treatment of child illness with antibiotics IMCI Intro/Planning • more frequent administration of the first dose at the facility Improved drug Training of health ITNs , other family and availability, supervision, workers/follow up visits community interventions other health system improvements Improved quality of care in • improved efforts by health workers to educate caregivers on home treatment health facilities Improved careseeking, Improved household increased utilization compliance/care • increased knowledge among mothers about how to administer drugs correctly Improved health/nutrition
The principles of integrated care The IMCI guidelines are based on the following principles: # All sick children must be examined for “general danger signs”. # All sick children must be routinely assessed for major symptoms # Only a limited number of carefully-selected clinical signs are used, based on evidence of their sensitivity and specificity7 to detect disease.
The road to healthy Palestinian childhood Palestinian Experiences in IMCI
Implementation of IMCI involves three phases: • the introductory phase to ensure that key persons in MoH and other health services providers understand IMCI strategy . • the early implementation phase to plan and prepare for IMCI implementation . • the expansion phase includes efforts to increase access and to broaden the range of IMCI interventions.
Achievements:Introduction phase: • H.E MOH Minister approved to adopt IMCI strategy within the health system 2001. • Introduction of IMCI approach under PHC umbrella. • Attendance of Rabat-morocco meeting 1998. • Attendance of inter-country meeting for IMCI national coordinators Damascus, Syria July 1999 (3 participants) from Gaza & WB
Nomination of IMCI National coordinator and IMCI focal persons for GAZA and West Bank. • One day orientation meeting conducted (August 2000) both in GAZA and West Bank. (WHO), followed by: • Two days preliminary and adaptation workshop (August 2000) in GAZA and West Banks. (WHO) • Orientation meeting (UNICEF and Al Quds university). • abroad training: IMCI task force members trained in Egypt (2 participants from GS & WB). * Training key personnel in Syria (4 participants) from GS & WB (2001) including IMCI national coordinator and Local persons.
2 orientation meetings in Gaza (2001) • IMCI working group formulation (IMCI task force):- • 1- Adapting group • 2- Planning and implementation group • 3- Community and family practice group
Early Implementation Phase: • Developing of national strategy and plan. • Initiate districts were selected • Adaptation of the IMCI guidelines one for physicians and one for nurse and training materials to the local context , producing Palestinian (national adapted IMCI guidelines and training material packages , mother card, wall charts, recording , reporting, and follow up requirements.
Printing of Palestinian IMCI materials • 4 consensus workshops were conducted. • TOT training course (15 in GAZA) (30 in WB) • IMCI training courses were held as 337 physicians were trained (189 in GAZA, 148 in WB), and 138 nurses also already trained • Attending most of inter-country meetings, related to all IMCI COMMPONENT.
Attending of both IMCI facilitation and follow training course to reinforce IMCI skills for trainers • Adaptation of a special psychosocial guideline and package were finished but need revision and piloting. (generic) . • Completing the building and upgrading of 3 training centers for IMCI & Neonatal strategy's activities distributed to cover all provinces.
IMCI components under activation: • National child health policy initiative (NCHPI). • IMCI community component (CIMCI). • IMCI psychosocial component (generic in Palestine). • breast feeding and supplementary feeding counsel for infants and young children component. • Adapting IMCI curriculum for pre-service training at medical and nursing collages . • IMCI Follow up after training and ongoing supervising. • Scaling up the IMCI Training activities
IMCI partnership • UNICEF • WHO / EMRO • Other partners: • * safe the children • *
Constrains 1- Political instability 2- conflicts in management system of MOH . 3- The strike of the MOH STAFF. 4- FINANCAL CONSTRAINS ( direct payment via UNICEF). 5- Mobility restriction ( the need for vehicle). 6- Limited capacity of MOH to recruit /assign technical staffs for IMCI org. structure. 7- Disparity between WB &GS in organizational structure results in non identical training approach. 8- Evacuation of trained staffs from PHCcs by transferring them to hospitals beside the turnover of some .
Web Site • Palestine have a special web sit at WHO – EMRO • http://www.emro.who.int/cah/imci_implementation_pal.asp?country=Palestine
IMCI: Lessons learned • Pneumonia and diarrhoea remain diseases most often associated with child deaths • Under-nutrition is an important direct cause associated with mortality from common childhood illnesses • IMCI provides a valuable and systematic conceptual for improving child health services • Where a well-defined IMCI management structure was in place and relations with other programs defined, program management and implementation were efficient
IMCI: Lessons learned…cont • IMCI is largely funded by donor resources and few governments have allocated a substantial regular budget line to it • IMCI in pre-service training of medical and para-medical health professionals is well embraced in many countries, and considered a necessary way forward for sustainable implementation • Follow-up after training has been found very useful, identify problems in the health system, and contribute to the process of system improvements at peripheral level • Wherever investments were made to improve the health system, this has had positive results on the system and enhanced the perceived success of IMCI implementation
IMCI: Lessons learned…cont • Poor health worker motivation and high turn-over negatively affect IMCI implementation • Adapting the pre-set national plan to be more flexible by adopting a scientific specific annual plan, this will help to absorb unforeseen incidents and achieve actual implementation . • C-IMCI should be activated as soon as possible to sensitize the communities towards child health, and sensitize participating health staff about why and how to deal with communities. • Decentralization of management tasks towards district is a prerequisite to help local capacity building, to introduce and enhance expansion and to maximize the potential for sustainability
Lot’s of unanswered questions Thank You