Download
1 / 57
570 likes | 735 Views
FNA of the Thyroid. Lisa Kendrick BSc., RT Cytology, CT (ASCP) School of Diagnostic Cytology Diagnostic Services of Manitoba/ Health Sciences Centre. Introduction . Anatomy and histology Clinical presentation Procedure Specimen preparation Cytology Microscope session. Anatomy.

E N D
FNA of the Thyroid Lisa Kendrick BSc., RT Cytology, CT (ASCP) School of Diagnostic Cytology Diagnostic Services of Manitoba/ Health Sciences Centre
Introduction • Anatomy and histology • Clinical presentation • Procedure • Specimen preparation • Cytology • Microscope session
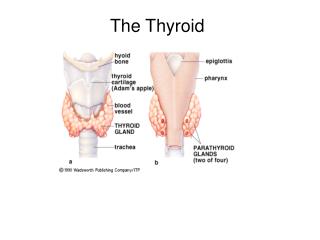
Anatomy • Located below the larynx • Consists of two lobes that lie on either side of the trachea • Lobes are connected by an ithmus • Is an endocrine gland • Concepts of Human Anatomy and Physiology, Van de Graff and Fox, page 504, Figure 19.13
Histology • Consists of spherical sacs – thyroid follicles • Lined by simple cuboidal epithelium • Contains colloid
Fine Needle Aspiration Procedure Fine Needle Biopsy of Thyroid Nodule
Preparation of Smears Smear Preparation
Follicular Cells • Nucleus • Central • Round/oval • Finely granular chromatin • 1 – 2 nucleoli • Cytoplasm • Pale • Indistinct • Arrangement • Honeycomb pattern
Satisfactory Specimen • 5 or more groups of 10 follicular cells each on a minimum of 2 slides (TBS)
Hurthle Cells • AKA Askanazy cells or Oncocytes • Large, polygonal cells • Nucleus • Round/oval • Eccentric • Finely granular chromatin • Cytoplasm • Abundant • Granular • Eosinophilic
Colloid • Found in the background • May stain blue, pink or metachromatic • Two states: • Watery Thick
Colloid Nodule • Most common form of goiter in adolescents and young women • Follicular cells cease to proliferate and colloid accumulates within the follicles
Colloid Nodule • Cytology • Macrofollicular pattern • Variable cellularity • Hurthle cell change may be seen • Scant follicular cells (normal in appearance) • Macrophages • Abundant colloid
Cystic Degeneration • FNA can cure 20 – 60% of cystic lesions by evacuation • Cytology • Few follicular cells • Abundant macrophages
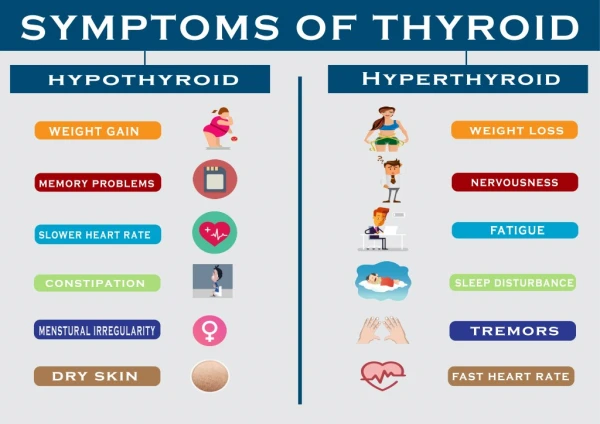
Hashimoto’s Thyroiditis • AKA chronic thyroiditis • An autoimmune disorder • Affects women more than men • Associated with hyperthyroidism
Hashimoto’s Thyroiditis Cytology • Cellular aspirate presenting in small groups, fragments • Groups of Hurthle cells • Follicular cells with Hurthle cell change • Inflammatory cells (lymphocytes and macrophages) • Tingible body macrophages • Little colloid • Possible lymphoma association
Follicular Carcinoma • Peak onset ages 40 through 60 • Females more common than males by 3 to 1 ratio • Prognosis directly related to tumor size [less than 1.0 cm (3/8 inch) good prognosis] • Rarely associated with radiation exposure • Spread to lymph nodes is uncommon (~10%) • Invasion into vascular structures (veins and arteries) within the thyroid gland is common • Distant spread (to lungs or bones) is uncommon, but more common than with papillary cancer • Overall cure rate high (near 95% for small lesions in young patients), decreases with advanced age • www.endocrineweb.com/capap.html
Follicular Carcinoma • Distinction between neoplasm and carcinoma depends on the histology specimen • Identification of invasion of either the capsule or blood vessels confirms the diagnosis of carcinoma • It is very difficult to differentiate between neoplasm and carcinoma based on morphology alone
Follicular Neoplasms • The cellularity varies • No colloid • Cells are arranged in small, loosely cohesive groups • Micro follicular pattern is observed • Syncytial patterns predominate • There may be overlap of some features with a colloid nodule
Follicular Neoplasm • Nucleus • Round • Smooth membrane • Fine/coarse even chromatin • Macronucleoli • Cytoplasm • Pale • Poorly defined
Papillary Carcinoma • Peak onset ages 30 through 50 • Females more common than males by 3 to 1 ratio • Prognosis directly related to tumor size [less than 1.5 cm (1/2 inch) good prognosis] • Accounts for 85% of thyroid cancers due to radiation exposure • Spread to lymph nodes of the neck present in more than 50% of cases • Distant spread (to lungs or bones) is very uncommon • Overall cure rate very high (near 100% for small lesions in young patients) • www.endocrineweb.com/capap.html
Papillary Carcinoma • Highly variable cellularity (very cellular to scant or cystic) • Little to no colloid • Papillary arrangements or monolayered fragments • Syncytia may be present • Enlarged polygonal cells
Papillary Carcinoma • Nucleus • Central • Overlapping • Round/oval/pleomorphic/ angulated • Finely granular (powdery) chromatin • Micro or macro nucleoli • Folds and creases (grooves) • Cytoplasmic nuclear inclusions • Abundant cytoplasm • Psammoma bodies may be present • Multinucleated macrophages
Hurthle Cell Neoplasm • Cellularity varies • Little to no colloid • Cells are dispersed or arranged in loose monolayers • May be follicular growth pattern • Monomorphic population of Hurthle cells • May have red macronucleoli • May demonstrate binucleation • May demonstrate nuclear grooving
Hurthle Cell Neoplasm • There is no clear separation between adenomas and carcinoma • However if the following features are present a carcinoma may be suspected: • Hypercellularity • Syncytia • Increased N:C • Nuclear pleomorphism • Multinucleoli
Medullary Carcinoma • Occurs in 4 clinical settings and can be associated with other endocrine tumors • Females more common than males (except for inherited cancers) • Regional metastases (spread to neck lymph nodes) occurs early in the disease • Spread to distant organs (metastasis) occurs late and can be to the liver, bone, brain, and adrenal medulla • Not associated with radiation exposure • Usually originates in the upper central lobe of the thyroid • Poor prognostic factors include age >50, male, distant spread (metastases), and when seen in patients with other endocrine tumors due to MEN II-B syndrome. • Residual disease (following surgery) or recurrence can be detected by measuring calcitonin (a hormone that should be measured every 4 months for the first few years and then every 6 months for ever). • www.endocrineweb.com/capap.html
4 Variants • Sporadic • MEN II-A (Sipple Syndrome) • MEN II-B • Inherited Medullary Carcinoma
Medullary Carcinoma • Not a common malignancy • Can be multifocal (in which the clinician may remove the entire thyroid) • Lymph node involvement is common
Medullary Carcinoma • Cellularity varies • Cell morphology varies • Plasmacytoid • Round • Polygonal • Spindle • Arranged in loose groups • Single cells are common • Amyloid may be present in the background
Medullary Carcinoma • Nuclei • Oval/pleomorphic • Coarse salt and pepper chromatin pattern • Central or eccentrically located • Indistinct nucleoli • Binucleation may be seen • Intranuclear inclusions may be seen • Cytoplasm is finely granular
Anaplastic Carcinoma • Very rare • Diagnosis is often suggested by clinical findings
Peak onset age 65 and older • Very rare in young patients • Females more common than in males • Typically presents as rapidly growing neck mass • Can occur many years after radiation exposure • Spread to lymph nodes of the neck present in more than 90% of cases • Distant spread (to lungs or bones) is very common even when first diagnosed • Overall cure rate very low • Typically requires a very aggressive treatment plan with surgery, radiation and sometimes even chemotherapy. • Often requires the patient to get a tracheostomy to maintain their airway. • www.endocrineweb.com/capap.html
Anaplastic Carcinoma • Giant or mixed forms • Variable cellularity • Inflammatory cells and necrotic debris are found in the background • Variable cell morphology • Squamoid • Giant cell • Spindle cell
Anaplastic Carcinoma • Nucleus • Pleomorphic in shape • Irregular membrane • Coarse, irregularly distributed chromatin • Prominent nucleoli • Atypical mitosis • Multinucleation • Cytoplasm • Densely granular
Metastatic Malignancies • Thyroid is a common site for metastases • Common metastatic tumors include: • Adenocarcinoma of the breast • Renal cell carcinoma • Squamous cell carcinoma from elsewhere • Melanoma • Lymphoma
Metastatic Melanoma • Cells are very pleomorphic • Pigment is often not present • Clinical history is very important • Immunohistochemistry aids in the diagnosis (S100, HMB45)
Lymphoma • Non-Hodgkin’s Hodgkin’s • monotonous population - Lymphoid cells and of lymphoid cells Reed-Sternberg cells
Surgery • Two types • 1. Lobectomy • The entire thyroid is removed. • 2. Hemithyroidectomy (lobectomy): • The surgeon removes the entire lobe on the side of the thyroid where the growth or cancer is found. If a biopsy of the growth confirms cancer, the surgeon may also remove the other lobe.
Radiation Therapy • Three types of radiation therapy: • 1. External beam radiation therapy - In external beam radiation therapy, radiation is directed at the cancer and surrounding tissue from a machine outside the body. It is used to treat most types of cancer. • 2. Brachytherapy - treats the cancer with a high total dose of radiation in a concentrated area in a short period of time. Sealed radioactive sources are placed in the body, in or near the cancer. A sealed radioactive source is often called an implant. • 3. Systemic radiation therapy - the radiation source is given as a liquid (either as a drink or in capsules that are swallowed) or by injecting it into a vein (an intravenous injection). The radiation source travels throughout the body.